

Differentiation of hemorrhage from iodinated contrast in different intracranial compartments using dual-energy head CT
- PMID: 22268092
- PMCID: PMC8013231
- DOI: 10.3174/ajnr.A2909
Differentiation of hemorrhage from iodinated contrast in different intracranial compartments using dual-energy head CT
Abstract
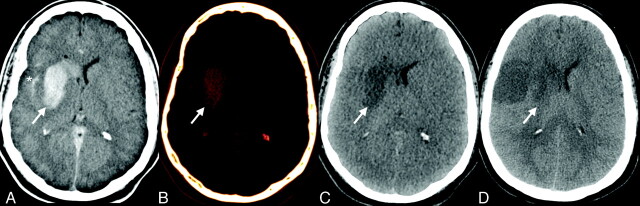
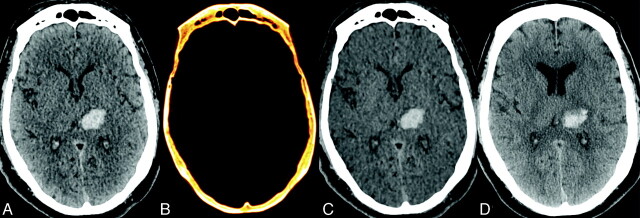
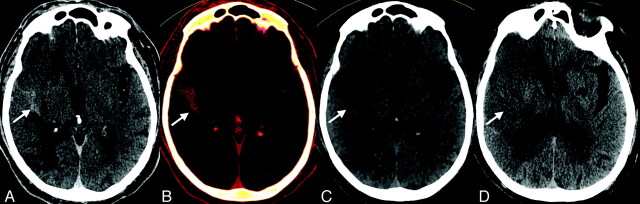
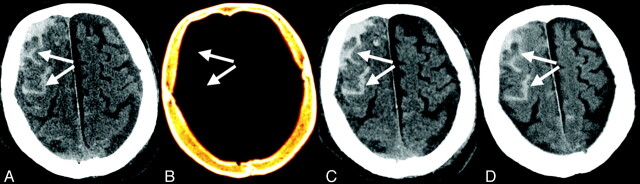
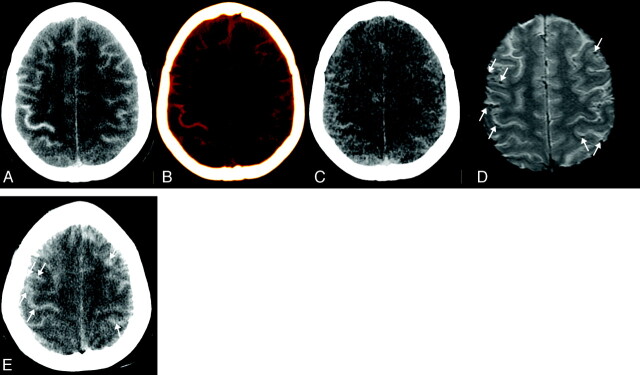
Background and purpose: Identification of ICH, particularly after ischemic stroke therapy, is important for guiding subsequent antithrombotic management and is often confounded by contrast staining or extravasations within intracerebral or extra-axial compartments. This study evaluates the accuracy of DECT in distinguishing ICH from iodinated contrast in patients who received contrast via IA or IV delivery.
Materials and methods: Forty patients who had received IA or IV contrast were evaluated using a DECT scanner at 80kV and 140kV to distinguish hyperdensities secondary to contrast staining or extravasation from those representing ICH. A 3-material decomposition algorithm was used to obtain virtual noncontrast images and iodine overlay images. Sensitivity, specificity, and accuracy of DECT in prospectively distinguishing intracranial contrast from hemorrhage within parenchymal, subarachnoid, extra-axial, intraventricular, and intra-arterial compartments were computed using routine clinical follow-up imaging as the standard of reference.
Results: A total of 148 foci of intracranial hyperattenuation were identified. Of these, 142 were correctly classified for the presence of hemorrhage by DECT. The sensitivity, specificity, and accuracy for identifying hemorrhage, depending on the compartment being considered, were 100%, 84.4%-100%, and 87.2%-100%, respectively. The only instances where DECT failed to correctly identify the source of hyperattenuation was in the presence of diffuse parenchymal calcification (n = 5) and a metallic streak artifact (n = 1).
Conclusion: After IA and/or IV contrast administration, DECT can accurately differentiate all types of ICH from iodinated contrast without employing any additional radiation.
Figures
References
-
- Mericle RA, Lopes DK, Fronckowiak MD, et al. A grading scale to predict outcomes after intra-arterial thrombolysis for stroke complicated by contrast extravasation. Neurosurgery 2000;46:1307–14; discussion 1314-15 - PubMed
-
- Greer DM, Koroshetz WJ, Cullen S, et al. Magnetic resonance imaging improves detection of intracerebral hemorrhage over computed tomography after intra-arterial thrombolysis. Stroke 2004;35:491–95 - PubMed
-
- Graser A, Johnson TR, Chandarana H, et al. Dual energy CT: preliminary observations and potential clinical applications in the abdomen. Eur Radiol 2009;19:13–23 - PubMed
-
- Ferda J, Novak M, Mirka H, et al. The assessment of intracranial bleeding with virtual unenhanced imaging by means of dual-energy CT angiography. Eur Radiol 2009;19:2518–22 - PubMed
-
- Gupta R, Phan CM, Leidecker C, et al. Evaluation of dual-energy CT for differentiating intracerebral hemorrhage from iodinated contrast material staining. Radiology 2010;257:205–11 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical