

Long-term survival of patients with ischemic cardiomyopathy treated by coronary artery bypass grafting versus medical therapy
- PMID: 22269720
- PMCID: PMC3638256
- DOI: 10.1016/j.athoracsur.2011.10.064
Long-term survival of patients with ischemic cardiomyopathy treated by coronary artery bypass grafting versus medical therapy
Abstract
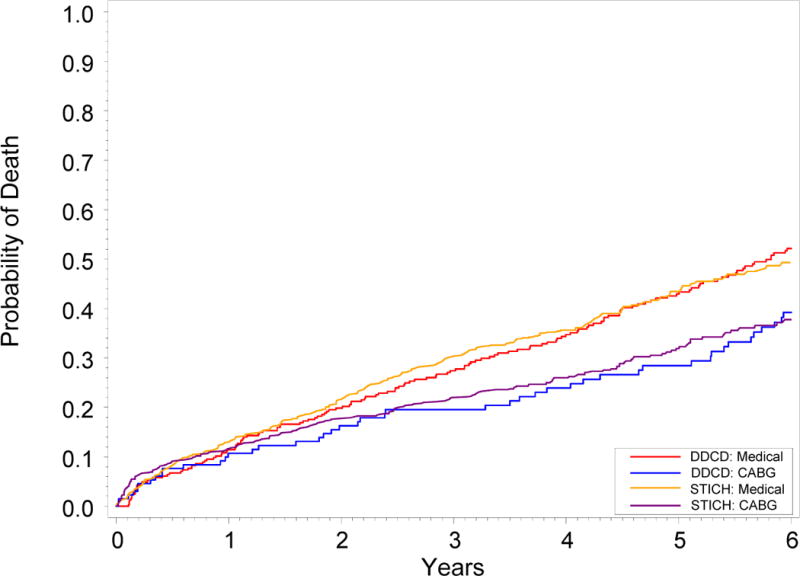
Background: We prospectively applied the Surgical Treatment of Ischemic Cardiomyopathy trial entry criteria to an observational database to determine whether coronary artery bypass grafting (CABG) decreases mortality compared with medical therapy (MED) for patients with coronary artery disease and depressed left ventricular ejection fraction.
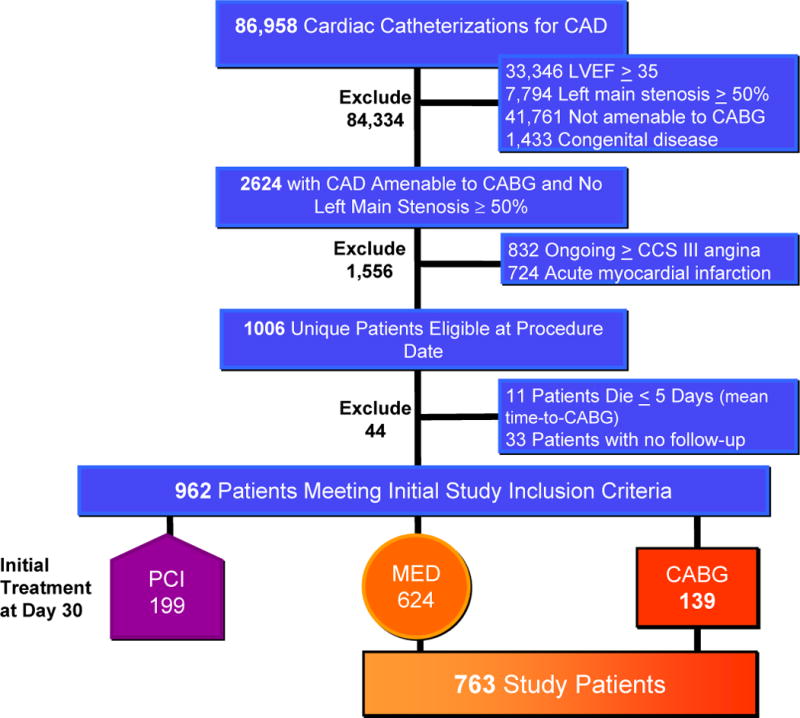
Methods: This was a retrospective, observational, cohort study of prospectively collected data from the Duke Databank for Cardiovascular Disease. Long-term mortality was the main outcome measure. Between January 1, 1995, and July 31, 2009, 86,874 patients underwent cardiac catheterization for suspected ischemic heart disease and were evaluated for inclusion in the analysis.
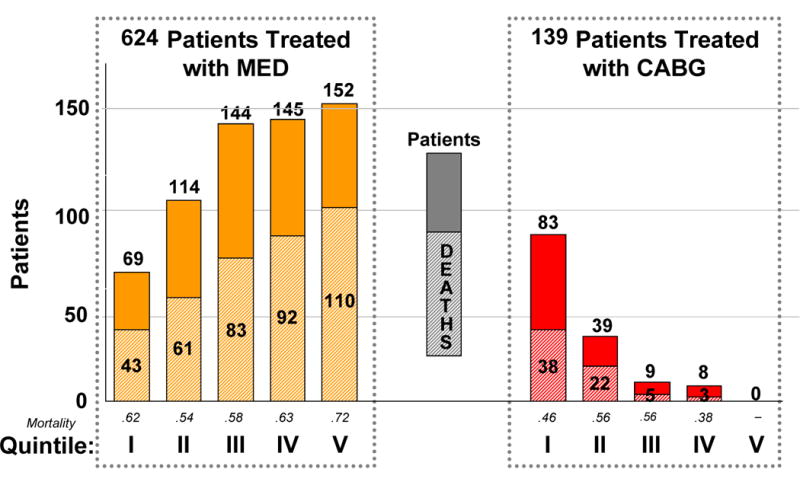
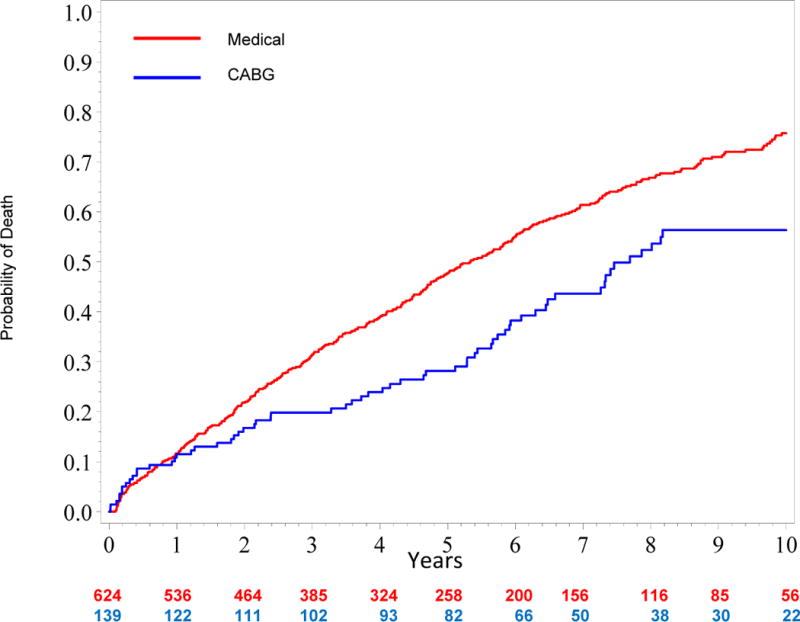
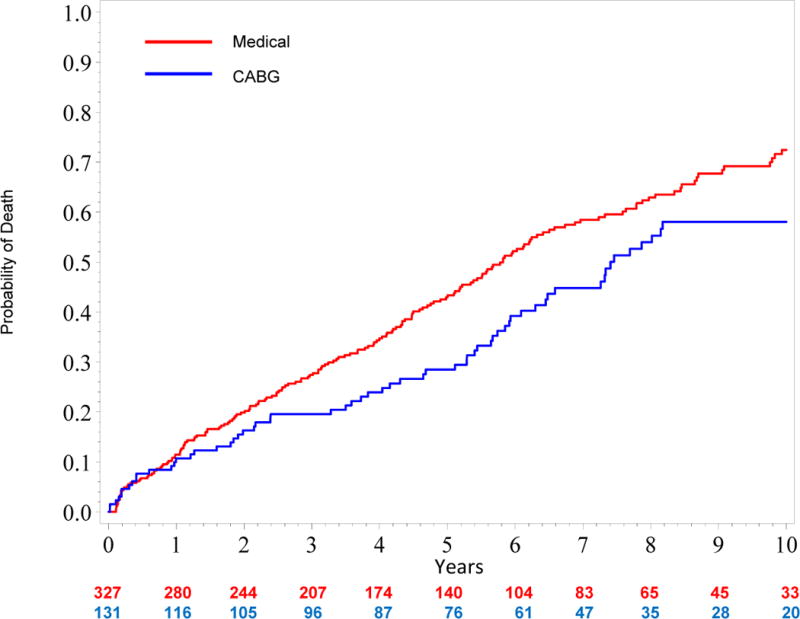
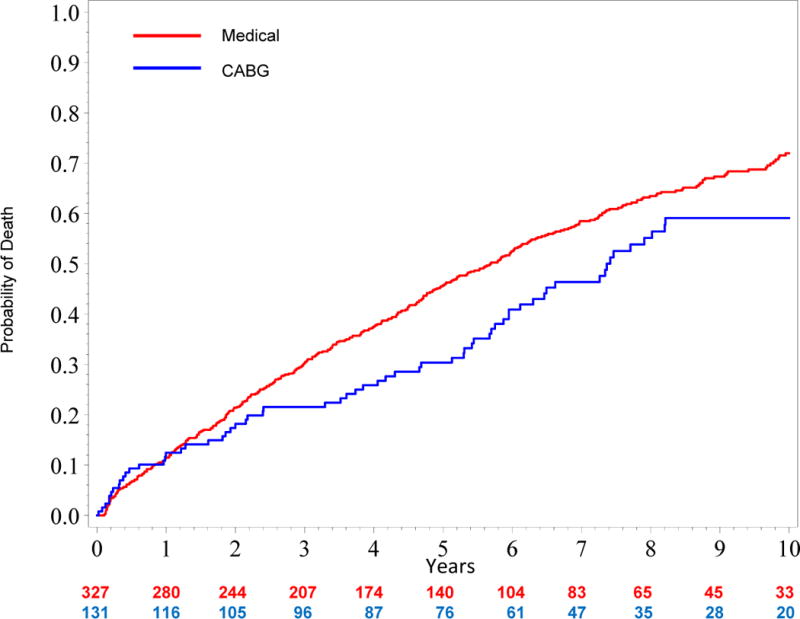
Results: A total of 2,624 patients were found to have left ventricular ejection fraction less than 0.35, coronary artery disease amenable to CABG, and no left main stenosis of greater than 50%. After exclusions including ongoing Canadian Cardiovascular Society class III angina and acute myocardial infarction, 763 patients were included for propensity score analysis, including 624 who received MED and 139 who underwent CABG. Adjusted mortality curves were constructed for those patients in the three quintiles most likely to receive CABG. The curves diverged early, with risk-adjusted mortality rates at 5 years of 46% for MED versus 29% for CABG, and the survival benefit of CABG over MED continued through 10 years of follow-up (hazard ratio, 0.63; 95% confidence interval, 0.45 to 0.88).
Conclusions: Among a propensity-matched, risk-adjusted, observational cohort of patients with coronary artery disease, left ventricular ejection fraction less than 0.35, and no left main disease of greater than 50%, CABG is associated with a survival advantage over MED through 10 years of follow-up.
Copyright © 2012 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invited commentary.Ann Thorac Surg. 2012 Feb;93(2):530. doi: 10.1016/j.athoracsur.2011.10.075. Ann Thorac Surg. 2012. PMID: 22269721 No abstract available.
References
-
- Hunt S, Abraham WT, Chin MH, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119(14):391–479. - PubMed
-
- Jessup M, Brozema S. Heart Failure. N Engl J Med. 2003;348:2007–2018. - PubMed
-
- Baker D, Jones R, Hodges J, et al. Management of Heart Failure. III. The role of revascularization in the treatment of patients with moderate or severe left ventricular systolic dysfunction. JAMA. 1994;272:1158–1134. - PubMed
-
- Ghali J, Kadakia S, Cooper R, et al. Precipitating factors leading to decompensation of heart failure. Arch Intern Med. 1988;148:2013–2016. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
