

Comparison of embedded and added motor imagery training in patients after stroke: results of a randomised controlled pilot trial
- PMID: 22269834
- PMCID: PMC3316146
- DOI: 10.1186/1745-6215-13-11
Comparison of embedded and added motor imagery training in patients after stroke: results of a randomised controlled pilot trial
Abstract
Background: Motor imagery (MI) when combined with physiotherapy can offer functional benefits after stroke. Two MI integration strategies exist: added and embedded MI. Both approaches were compared when learning a complex motor task (MT): 'Going down, laying on the floor, and getting up again'.
Methods: Outpatients after first stroke participated in a single-blinded, randomised controlled trial with MI embedded into physiotherapy (EG1), MI added to physiotherapy (EG2), and a control group (CG). All groups participated in six physiotherapy sessions. Primary study outcome was time (sec) to perform the motor task at pre and post-intervention.
Secondary outcomes: level of help needed, stages of MT-completion, independence, balance, fear of falling (FOF), MI ability. Data were collected four times: twice during one week baseline phase (BL, T0), following the two week intervention (T1), after a two week follow-up (FU). Analysis of variance was performed.
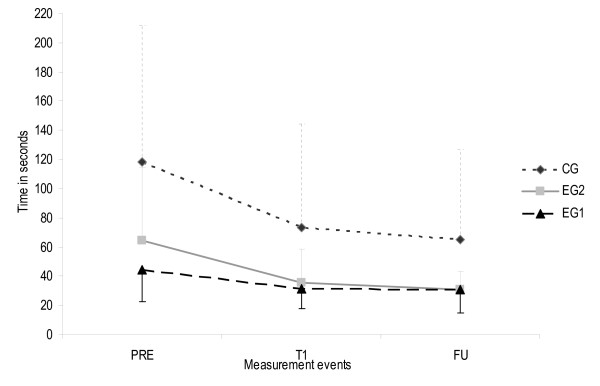
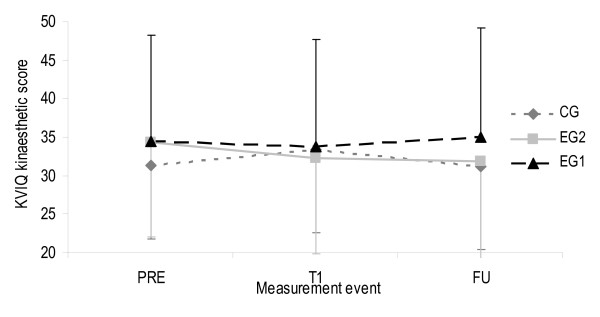
Results: Thirty nine outpatients were included (12 females, age: 63.4 ± 10 years; time since stroke: 3.5 ± 2 years; 29 with an ischemic event). All were able to complete the motor task using the standardised 7-step procedure and reduced FOF at T0, T1, and FU. Times to perform the MT at baseline were 44.2 ± 22s, 64.6 ± 50s, and 118.3 ± 93s for EG1 (N = 13), EG2 (N = 12), and CG (N = 14). All groups showed significant improvement in time to complete the MT (p < 0.001) and degree of help needed to perform the task: minimal assistance to supervision (CG) and independent performance (EG1+2). No between group differences were found. Only EG1 demonstrated changes in MI ability over time with the visual indicator increasing from T0 to T1 and decreasing from T1 to FU. The kinaesthetic indicator increased from T1 to FU. Patients indicated to value the MI training and continued using MI for other difficult-to-perform tasks.
Conclusions: Embedded or added MI training combined with physiotherapy seem to be feasible and benefi-cial to learn the MT with emphasis on getting up independently. Based on their baseline level CG had the highest potential to improve outcomes. A patient study with 35 patients per group could give a conclusive answer of a superior MI integration strategy.
Trial registration: ClinicalTrials.gov: NCT00858910.
Figures











References
-
- Page SJ. Imagery improves upper extremity motor function in chronic stroke patients: a pilot study. Occup Ther J Res. 2000;20(3):200–215.
-
- Page SJ, Levine P, Sisto SA, Johnston MV. Mental practice combined with physical practice for upper-limb motor deficit in subacute stroke. Phys Ther. 2001;81(8):1455–1462. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
