

Nodal metastasis risk in endometrioid endometrial cancer
- PMID: 22270280
- PMCID: PMC3266531
- DOI: 10.1097/AOG.0b013e318240de51
Nodal metastasis risk in endometrioid endometrial cancer
Abstract
Objective: To estimate the risk for nodal metastasis in women with endometrial cancer based on uterine characteristics on pathology.
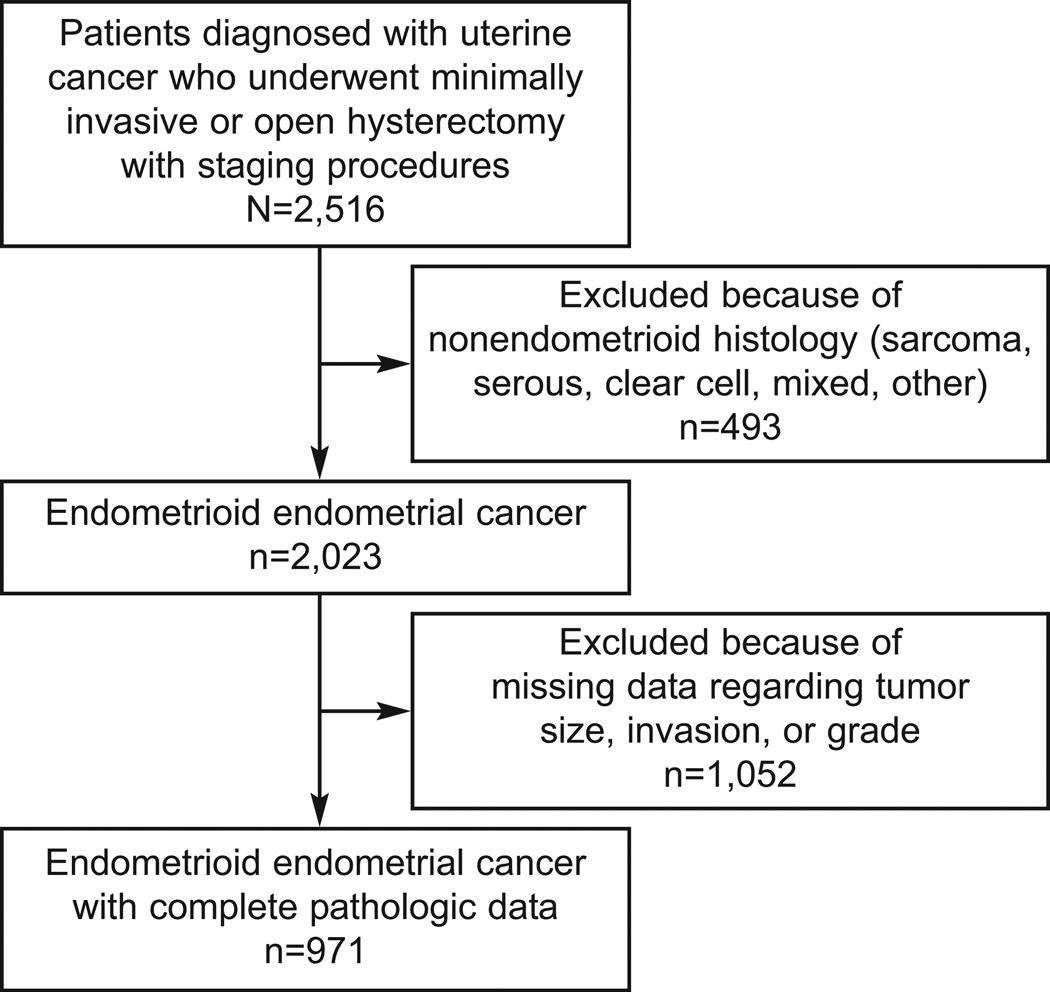
Methods: From a study of staging for uterine cancer, women were identified as being at low risk for nodal metastasis based on three specific criteria on final pathology reports: 1) less than 50% invasion, 2) tumor size less than 2 cm, and 3) well or moderately differentiated endometrioid histology. If the uterine specimen did not meet all three criteria, it was viewed as high risk for nodal metastasis.
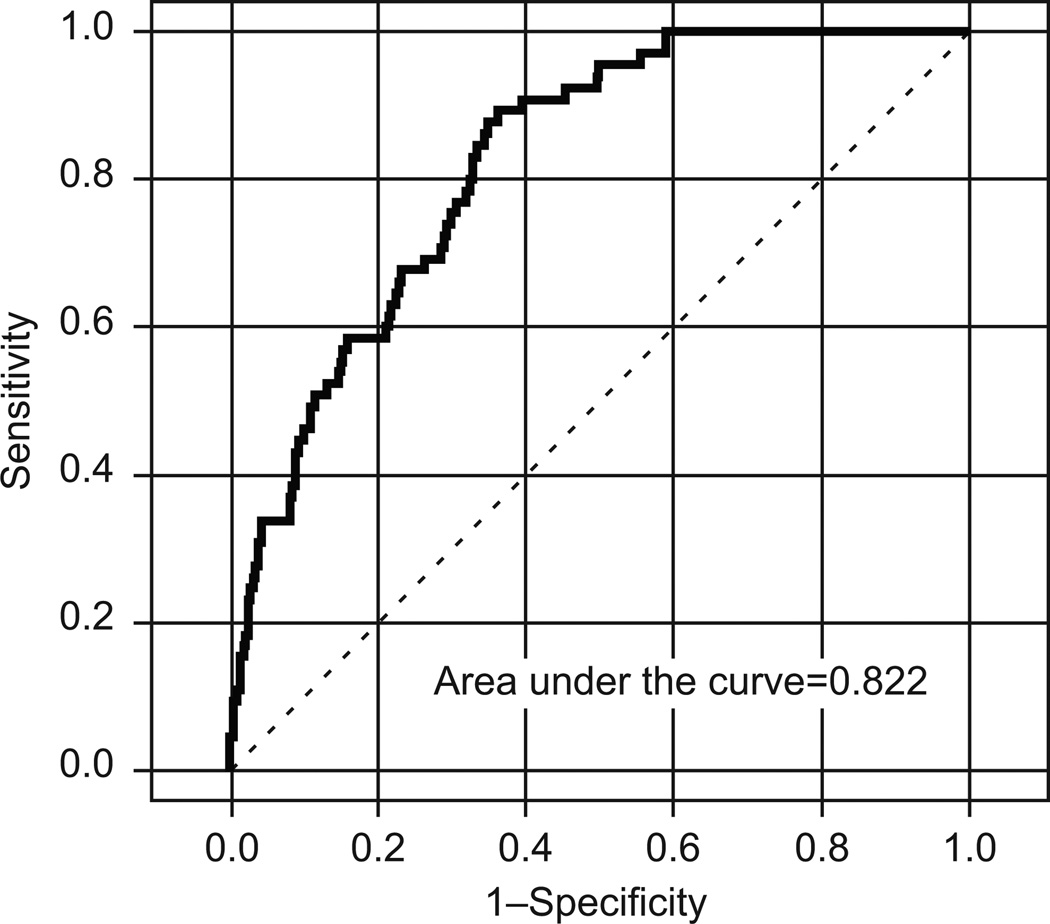
Results: Nine hundred seventy-one women were included in this analysis. Approximately 40% (or 389 of 971) of patients in this study were found to be at low risk, with a rate of nodal metastasis of only 0.8% (3 of 389; exact 95% confidence interval [CI] 0.16-2.2). No statistical differences in median age, body mass index, race, performance status, missing clinical data, or open or minimally invasive techniques were found among the patients with and without nodal metastases. Patients with high-risk characteristics of their uterine specimens compared with those with low-risk characteristics have 6.3 times the risk of nodal metastasis (95% CI 1.67-23.8, P=.007).
Conclusion: Low-risk endometrioid uterine cancer criteria may be used to help guide treatment planning for reoperation in patients with incomplete surgical staging information.
Level of evidence: II.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Creasman WT, Morrow CP, Bundy BN, Homesley HD, Graham JE, Heller PB. Surgical pathologic spread patterns of endometrial cancer. A Gynecologic Oncology Group Study. Cancer. 1987;60:2035–2041. - PubMed
-
- Schink JC, Lurain JR, Wallemark CB, Chmiel JS. Tumor size in endometrial cancer: a prognostic factor for lymph node metastasis. Obstet Gynecol. 1987;70:216–219. - PubMed
-
- Mariani A, Webb MJ, Keeney GL, et al. Low-risk corpus cancer: is lymphadenectomy or radiotherapy necessary? Am J Obstet Gynecol. 2000;182:1506–1519. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
