

Pharmacological and nonpharmacological management of delirium in critically ill patients
- PMID: 22270810
- PMCID: PMC3271151
- DOI: 10.1007/s13311-011-0102-9
Pharmacological and nonpharmacological management of delirium in critically ill patients
Abstract
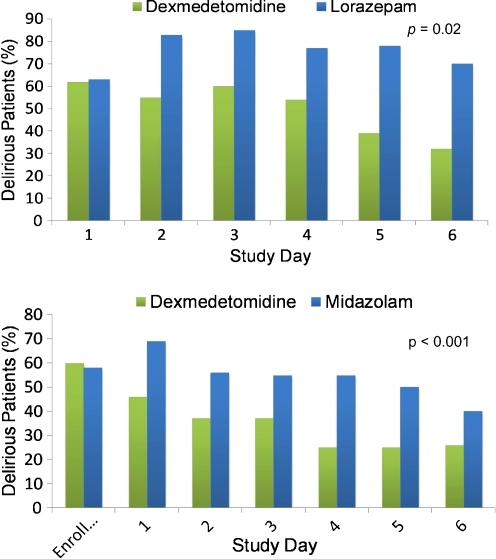
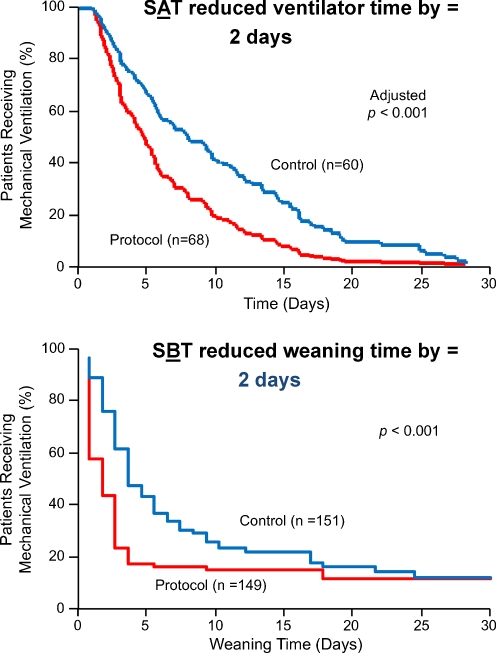
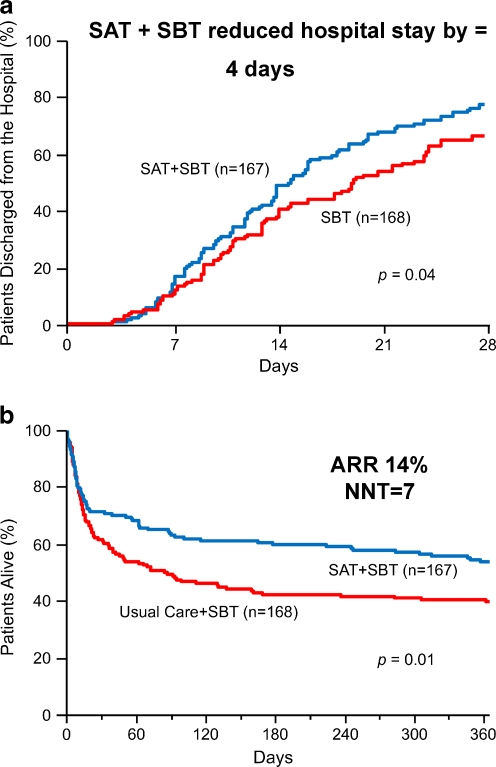
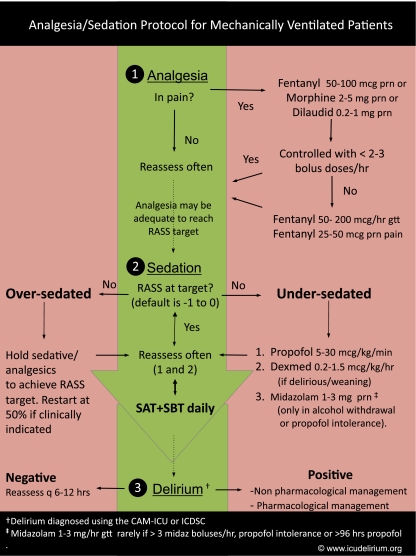
Delirium is a common yet under-diagnosed syndrome of acute brain dysfunction, which is characterized by inattention, fluctuating mental status, altered level of consciousness, or disorganized thinking. Although our recognition of risk factors for delirium has progressed, our understanding of the underlying pathophysiologic mechanisms remains limited. Improvements in monitoring and assessment for delirium (particularly in the intensive care setting) have resulted in validated and reliable tools such as arousal scales and bedside delirium monitoring instruments. Once delirium is recognized and the modifiable risk factors are addressed, the next step in management (if delirium persists) is often pharmacological intervention. The sedatives, analgesics, and hypnotics most often used in the intensive care unit (ICU) to achieve patient comfort are all too frequently deliriogenic, resulting in a longer duration of ICU and hospital stay, and increased costs. Therefore, identification of safe and efficacious agents to reduce the incidence, duration, and severity of ICU delirium is a hot topic in critical care. Recognizing that there are no medications approved by the Food and Drug Administration (FDA) for the prevention or treatment of delirium, we chose anti-psychotics and alpha-2 agonists as the general pharmacological focus of this article because both were subjects of relatively recent data and ongoing clinical trials. Emerging pharmacological strategies for addressing delirium must be combined with nonpharmacological approaches (such as daily spontaneous awakening trials and spontaneous breathing trials) and early mobility (combined with the increasingly popular approach called: Awakening and Breathing Coordination, Delirium Monitoring, Early Mobility, and Exercise [ABCDE] of critical care) to develop evidence-based approaches that will ensure safer and faster recovery of the sickest patients in our healthcare system.
Figures
References
-
- Verghese A. Cutting for Stone. First Vintage Books Edition. New York: Vintage Books; 2009.
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA. 2004;291:1753–1762. - PubMed
-
- Lin SM, Liu CY, Wang CH, et al. The impact of delirium on the survival of mechanically ventilated patients. Crit Care Med. 2004;32:2254–2259. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
