

Modeling cardiac electromechanics and mechanoelectrical coupling in dyssynchronous and failing hearts: insight from adaptive computer models
- PMID: 22271009
- PMCID: PMC3294221
- DOI: 10.1007/s12265-012-9346-y
Modeling cardiac electromechanics and mechanoelectrical coupling in dyssynchronous and failing hearts: insight from adaptive computer models
Abstract
Computer models have become more and more a research tool to obtain mechanistic insight in the effects of dyssynchrony and heart failure. Increasing computational power in combination with increasing amounts of experimental and clinical data enables the development of mathematical models that describe electrical and mechanical behavior of the heart. By combining models based on data at the molecular and cellular level with models that describe organ function, so-called multi-scale models are created that describe heart function at different length and time scales. In this review, we describe basic modules that can be identified in multi-scale models of cardiac electromechanics. These modules simulate ionic membrane currents, calcium handling, excitation-contraction coupling, action potential propagation, and cardiac mechanics and hemodynamics. In addition, we discuss adaptive modeling approaches that aim to address long-term effects of diseases and therapy on growth, changes in fiber orientation, ionic membrane currents, and calcium handling. Finally, we discuss the first developments in patient-specific modeling. While current models still have shortcomings, well-chosen applications show promising results on some ultimate goals: understanding mechanisms of dyssynchronous heart failure and tuning pacing strategy to a particular patient, even before starting the therapy.
Figures


Similar articles
-
Electromechanical models of the ventricles.Am J Physiol Heart Circ Physiol. 2011 Aug;301(2):H279-86. doi: 10.1152/ajpheart.00324.2011. Epub 2011 May 13. Am J Physiol Heart Circ Physiol. 2011. PMID: 21572017 Free PMC article.
-
Mechanistic insight into prolonged electromechanical delay in dyssynchronous heart failure: a computational study.Am J Physiol Heart Circ Physiol. 2013 Oct 15;305(8):H1265-73. doi: 10.1152/ajpheart.00426.2013. Epub 2013 Aug 9. Am J Physiol Heart Circ Physiol. 2013. PMID: 23934857 Free PMC article.
-
Multi-scale modeling of excitation-contraction coupling in the normal and failing heart.Annu Int Conf IEEE Eng Med Biol Soc. 2009;2009:4281-2. doi: 10.1109/IEMBS.2009.5332708. Annu Int Conf IEEE Eng Med Biol Soc. 2009. PMID: 19963818 Free PMC article.
-
[Mathematical models for the study of electromechanical and mechanoelectrical coupling in the myocardium].Ross Fiziol Zh Im I M Sechenova. 2007 Sep;93(9):945-68. Ross Fiziol Zh Im I M Sechenova. 2007. PMID: 18030795 Review. Russian.
-
Modeling the cellular basis of altered excitation-contraction coupling in heart failure.Prog Biophys Mol Biol. 1998;69(2-3):497-514. doi: 10.1016/s0079-6107(98)00022-4. Prog Biophys Mol Biol. 1998. PMID: 9785953 Review.
Cited by
-
Towards Personalized Cardiology: Multi-Scale Modeling of the Failing Heart.PLoS One. 2015 Jul 31;10(7):e0134869. doi: 10.1371/journal.pone.0134869. eCollection 2015. PLoS One. 2015. PMID: 26230546 Free PMC article.
-
Mathematical modeling and simulation of ventricular activation sequences: implications for cardiac resynchronization therapy.J Cardiovasc Transl Res. 2012 Apr;5(2):146-58. doi: 10.1007/s12265-011-9343-6. Epub 2012 Jan 27. J Cardiovasc Transl Res. 2012. PMID: 22282106 Free PMC article. Review.
-
Dynamic finite-strain modelling of the human left ventricle in health and disease using an immersed boundary-finite element method.IMA J Appl Math. 2014 Oct;79(5):978-1010. doi: 10.1093/imamat/hxu029. Epub 2014 Jul 1. IMA J Appl Math. 2014. PMID: 27041786 Free PMC article.
-
Excitation-contraction coupling between human atrial myocytes with fibroblasts and stretch activated channel current: a simulation study.Comput Math Methods Med. 2013;2013:238676. doi: 10.1155/2013/238676. Epub 2013 Aug 13. Comput Math Methods Med. 2013. PMID: 24000290 Free PMC article.
-
Mechanical discoordination increases continuously after the onset of left bundle branch block despite constant electrical dyssynchrony in a computational model of cardiac electromechanics and growth.Europace. 2012 Nov;14 Suppl 5(Suppl 5):v65-v72. doi: 10.1093/europace/eus274. Europace. 2012. PMID: 23104917 Free PMC article.
References
-
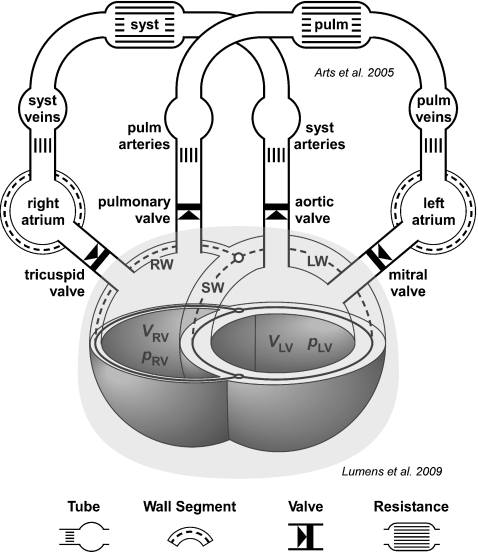
- Arts T, Delhaas T, Bovendeerd P, Verbeek X, Prinzen FW. Adaptation to mechanical load determines shape and properties of heart and circulation: The Circ-Adapt model. American Journal of Physiology. Heart and Circulatory Physiology. 2005;288:H1943–H1954. doi: 10.1152/ajpheart.00444.2004. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
