

Trends in physician referrals in the United States, 1999-2009
- PMID: 22271124
- PMCID: PMC3568395
- DOI: 10.1001/archinternmed.2011.722
Trends in physician referrals in the United States, 1999-2009
Abstract
Background: Physician referrals play a central role in ambulatory care in the United States; however, little is known about national trends in physician referrals over time. The objective of this study was to assess changes in the annual rate of referrals to other physicians from physician office visits in the United States from 1999 to 2009.
Methods: We analyzed nationally representative cross-sections of ambulatory patient visits in the United States, using a sample of 845 243 visits from the National Ambulatory Medical Care Survey and National Hospital Ambulatory Medical Care Survey from 1993 to 2009, focusing on the decade from 1999 to 2009. The main outcome measures were survey-weighted estimates of the total number and percentage of visits resulting in a referral to another physician across several patient and physician characteristics.
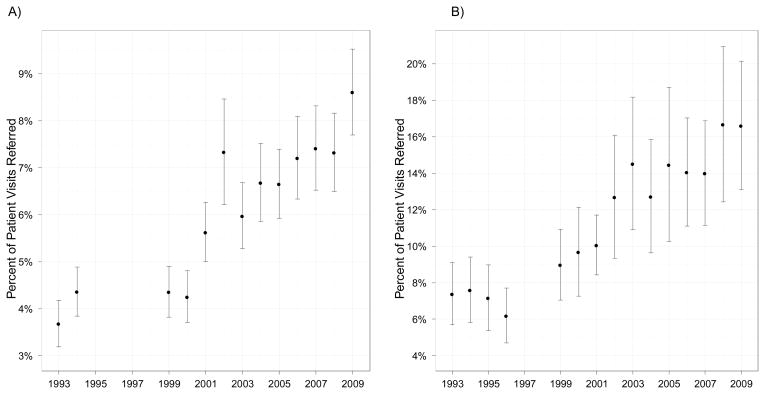
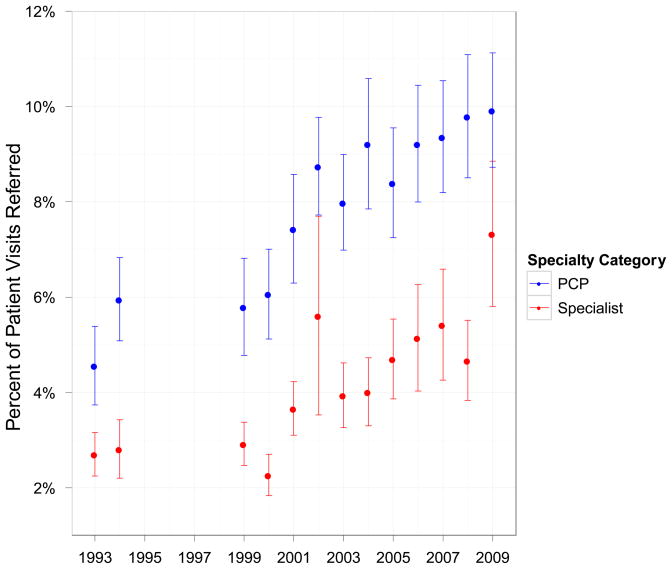
Results: From 1999 to 2009, the probability that an ambulatory visit to a physician resulted in a referral to another physician increased from 4.8% to 9.3% (P < .001), a 94% increase. The absolute number of visits resulting in a physician referral increased 159% nationally during this time, from 41 million to 105 million. This trend was consistent across all subgroups examined, except for slower growth among physicians with ownership stakes in their practice (P = .02) or those with the majority of income from managed care contracts (P = .007). Changes in referral rates varied according to the principal symptoms accounting for patients' visits, with significant increases noted for visits to primary care physicians from patients with cardiovascular, gastrointestinal, orthopedic, dermatologic, and ear/nose/throat symptoms.
Conclusions: The percentage and absolute number of ambulatory visits resulting in a referral in the United States grew substantially from 1999 to 2009. More research is necessary to understand the contribution of rising referral rates to costs of care.
Conflict of interest statement
The authors have no financial conflicts of interest to disclose.
Figures
Comment in
-
How can we know so little about physician referrals?Arch Intern Med. 2012 Jan 23;172(2):100. doi: 10.1001/archinternmed.2011.1290. Arch Intern Med. 2012. PMID: 22271117 No abstract available.
References
-
- Glenn JK, Lawler FH, Hoerl MS. Physician referrals in a competitive environment. An estimate of the economic impact of a referral. JAMA. 1987 Oct 9;258(14):1920–1923. - PubMed
-
- Boulware LE, Troll MU, Jaar BG, Myers DI, Powe NR. Identification and referral of patients with progressive CKD: a national study. Am J Kidney Dis. 2006 Aug;48(2):192–204. - PubMed
-
- Wu AW, Young Y, Skinner EA, et al. Quality of care and outcomes of adults with asthma treated by specialists and generalists in managed care. Archives of internal medicine. 2001 Nov 26;161(21):2554–2560. - PubMed
-
- Donohoe MT. Comparing generalist and specialty care: discrepancies, deficiencies, and excesses. Archives of internal medicine. 1998 Aug 10–24;158(15):1596–1608. - PubMed
-
- Greenfield S, Nelson EC, Zubkoff M, et al. Variations in resource utilization among medical specialties and systems of care. Results from the medical outcomes study. JAMA. 1992 Mar 25;267(12):1624–1630. - PubMed
