

Nonalcoholic fatty liver disease is associated with coronary artery calcification
- PMID: 22271511
- PMCID: PMC3830979
- DOI: 10.1002/hep.25593
Nonalcoholic fatty liver disease is associated with coronary artery calcification
Abstract
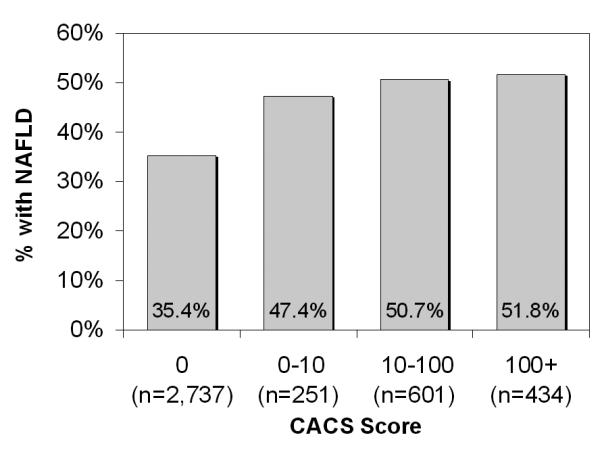
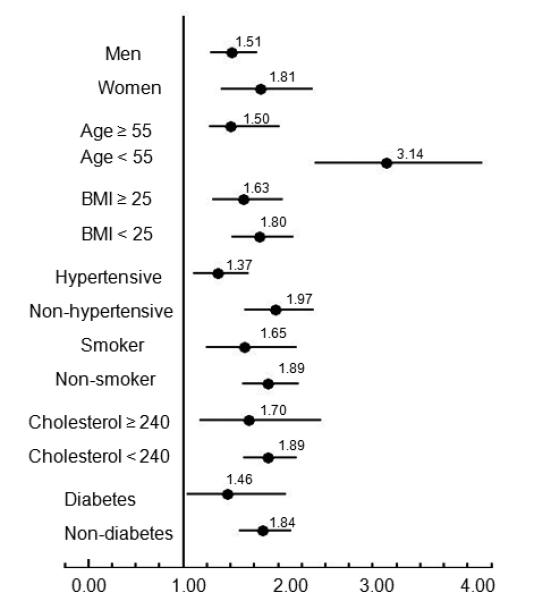
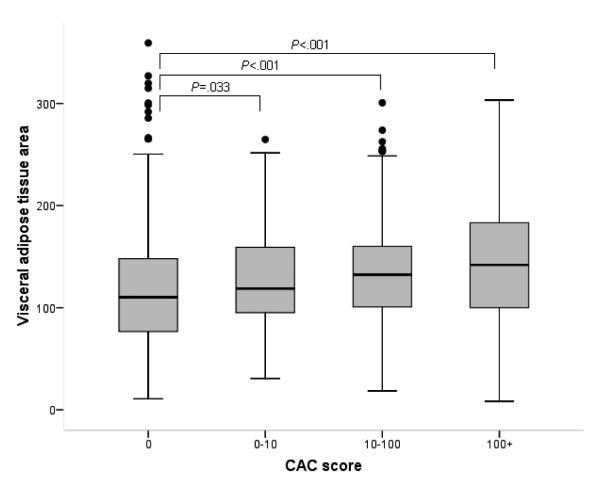
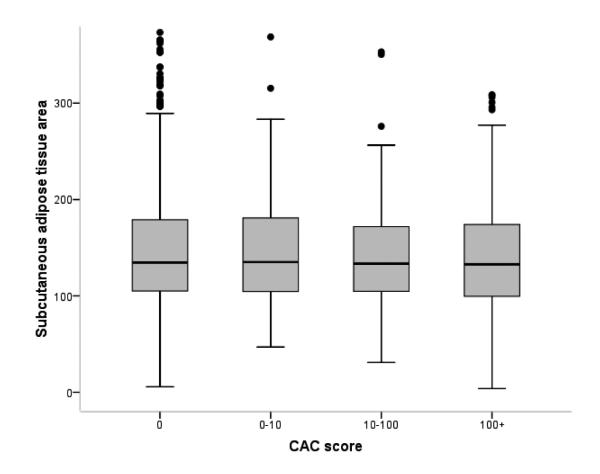
Nonalcoholic fatty liver disease (NAFLD) is related to risk factors of coronary artery disease, such as dyslipidemia, diabetes, and metabolic syndrome, which are closely linked with visceral adiposity. The aim of this study was to investigate whether NAFLD was associated with coronary artery calcification (CAC), which is used as a surrogate marker for coronary atherosclerosis independent of computed tomography (CT)-measured visceral adiposity. Out of 5,648 subjects who visited one of our health screening centers between 2003 and 2008, we enrolled 4,023 subjects (mean age, 56.9 ± 9.4 years; 60.7% males) without known liver disease or a history of ischemic heart disease. CAC score was evaluated using the Agatston method. On univariate analysis, the presence of CAC (score >0) was significantly associated with age, sex, body mass index, aspartate aminotransferase, alanine aminotransferase, high-density lipoprotein cholesterol, triglycerides, and increased risk of diabetes, hypertension, smoking, and NAFLD. Increasing CAC scores (0, <10, 10-100, ≥ 100) were associated with higher prevalence of NAFLD (odds ratio [OR], 1.84; 95% confidence interval [CI], 1.61-2.10; P<0.001). Multivariable ordinal regression analysis was adjusted for traditional risk factors, and CT-measured visceral adipose tissue area in a subgroup of subjects showed that the increased CAC scores were significantly associated with the presence of NAFLD (OR, 1.28, 95% CI, 1.04-1.59; P = 0.023) independent of visceral adiposity.
Conclusion: Patients with NAFLD are at increased risk for coronary atherosclerosis independent of classical coronary risk factors, including visceral adiposity. These data suggest that NAFLD might be an independent risk factor for coronary artery disease.
Copyright © 2012 American Association for the Study of Liver Diseases.
Figures
Comment in
-
Cardiovascular phenotype of nonalcoholic fatty liver disease: hanging the paradigm about the role of distant toxic fat accumulation on vascular disease.Hepatology. 2012 Sep;56(3):1185-6. doi: 10.1002/hep.25785. Hepatology. 2012. PMID: 22505369 No abstract available.
References
-
- Browning JD, Szczepaniak LS, Dobbins R, Nuremberg P, Horton JD, Cohen JC, Grundy SM, et al. Prevalence of hepatic steatosis in an urban population in the United States: impact of ethnicity. Hepatology. 2004;40:1387–1395. - PubMed
-
- Marchesini G, Brizi M, Bianchi G, Tomassetti S, Bugianesi E, Lenzi M, McCullough AJ, et al. Nonalcoholic fatty liver disease: a feature of the metabolic syndrome. Diabetes. 2001;50:1844–1850. - PubMed
-
- Targher G, Marra F, Marchesini G. Increased risk of cardiovascular disease in non-alcoholic fatty liver disease: causal effect or epiphenomenon? Diabetologia. 2008;51:1947–1953. - PubMed
-
- Choi SY, Kim D, Kang JH, Park MJ, Kim YS, Lim SH, Kim CH, et al. Nonalcoholic fatty liver disease as a risk factor of cardiovascular disease: relation of non-alcoholic fatty liver disease to carotid atherosclerosis. Korean J Hepatol. 2008;14:77–88. - PubMed
-
- Brea A, Mosquera D, Martin E, Arizti A, Cordero JL, Ros E. Nonalcoholic fatty liver disease is associated with carotid atherosclerosis: a case-control study. Arterioscler Thromb Vasc Biol. 2005;25:1045–1050. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical