

Pooled analysis of a self-sampling HPV DNA Test as a cervical cancer primary screening method
- PMID: 22271765
- PMCID: PMC3274511
- DOI: 10.1093/jnci/djr532
Pooled analysis of a self-sampling HPV DNA Test as a cervical cancer primary screening method
Abstract
Background: Worldwide, one-seventh of cervical cancers occur in China, which lacks a national screening program. By evaluating the diagnostic accuracy of self-collected cervicovaginal specimens tested for human papillomavirus (HPV) DNA (Self-HPV testing) in China, we sought to determine whether Self-HPV testing may serve as a primary cervical cancer screening method in low-resource settings.
Methods: We compiled individual patient data from five population-based cervical cancer-screening studies in China. Participants (n = 13 140) received Self-HPV testing, physician-collected cervical specimens for HPV testing (Physician-HPV testing), liquid-based cytology (LBC), and visual inspection with acetic acid (VIA). Screen-positive women underwent colposcopy and confirmatory biopsy. We analyzed the accuracies of pooled Self-HPV testing, Physician-HPV testing, VIA, and LBC to detect biopsy-confirmed cervical intraepithelial neoplasia grade 2 or more severe (CIN2+) and CIN3+. All statistical tests were two-sided.
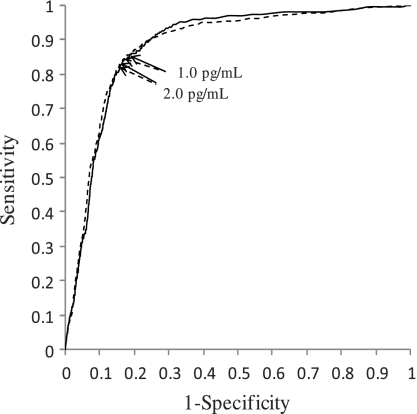
Results: Of 13 004 women included in the analysis, 507 (3.9%) were diagnosed as CIN2+, 273 (2.1%) as CIN3+, and 37 (0.3%) with cervical cancer. Self-HPV testing had 86.2% sensitivity and 80.7% specificity for detecting CIN2+ and 86.1% sensitivity and 79.5% specificity for detecting CIN3+. VIA had statistically significantly lower sensitivity for detecting CIN2+ (50.3%) and CIN3+ (55.7%) and higher specificity for detecting CIN2+ (87.4%) and CIN3+ (86.9%) (all P values < .001) than Self-HPV testing, LBC had lower sensitivity for detecting CIN2+ (80.7%, P = .015), similar sensitivity for detecting CIN3+ (89.0%, P = .341), and higher specificity for detecting CIN2+ (94.0%, P < .001) and CIN3+ (92.8%, P < .001) than Self-HPV testing. Physician-HPV testing was more sensitive for detecting CIN2+ (97.0%) and CIN3+ (97.8%) but similarly specific for detecting CIN2+ (82.7%) and CIN3+ (81.3%) (all P values <.001) than Self-HPV testing.
Conclusions: The sensitivity of Self-HPV testing compared favorably with that of LBC and was superior to the sensitivity of VIA. Self-HPV testing may complement current screening programs by increasing population coverage in settings that do not have easy access to comprehensive cytology-based screening.
Figures


Comment in
-
Is it time to introduce HPV self-sampling for primary cervical cancer screening?J Natl Cancer Inst. 2012 Feb 8;104(3):166-7. doi: 10.1093/jnci/djr544. Epub 2012 Jan 23. J Natl Cancer Inst. 2012. PMID: 22271766 No abstract available.
References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer. 2010;127(12):2893–2917. - PubMed
-
- International Agency for Research on Cancer (IARC) IARC Handbooks of Cancer Prevention: Cervix Cancer Screening, Chapter 2. Lyon, France: IARC Press; 2005.
-
- Belinson J, Qiao YL, Pretorius R, et al. Shanxi Province Cervical Cancer Screening Study: a cross-sectional comparative trial of multiple techniques to detect cervical neoplasia. Gynecol Oncol. 2001;83(2):439–444. - PubMed
-
- The Lancet. Women's health in rural China. Lancet. 2009;374(9687):358. - PubMed
-
- Cuzick J, Clavel C, Petry KU, et al. Overview of the European and North American studies on HPV testing in primary cervical cancer screening. Int J Cancer. 2006;119(5):1095–1101. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
