

Outcomes after the long interdialytic break: implications for the dialytic prescription
- PMID: 22273522
- PMCID: PMC3433739
- DOI: 10.1111/j.1525-139X.2011.01015.x
Outcomes after the long interdialytic break: implications for the dialytic prescription
Abstract
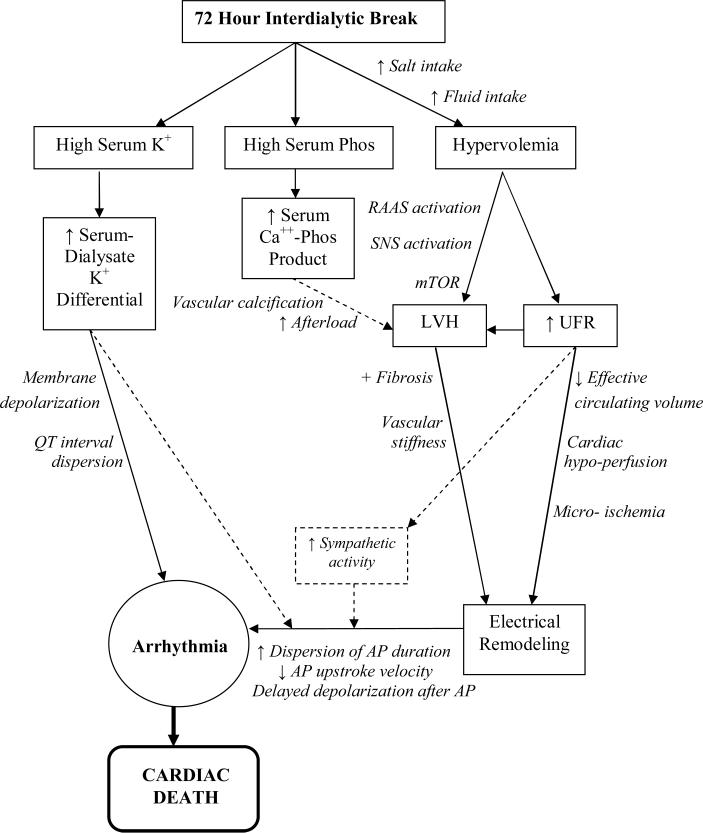
A thrice-weekly schedule dominates hemodialysis practice today. Inherent in such a schedule is a 72-hour interweek break over the weekend. A growing body of evidence suggests that this break may be associated with increased cardiovascular morbidity and mortality. Five recent studies have linked dialysis session timing to higher cardiovascular event rates, and have shed light on possible underlying physiologic mechanisms. We reviewed outcome data linking the "long break" to cardiovascular outcomes, and suggest physiologic rationale for this relationship while identifying knowledge gaps that require further study to inform discussions regarding the application and composition of individualized dialysis prescriptions. Further work is needed to determine the relative importance of electrolyte perturbations and hemodynamic shifts in the relationship between the long break and cardiovascular mortality. The evidence suggests that at least in some at-risk patients, an individualized approach to the dialytic schedule and prescription is warranted.
© 2012 Wiley Periodicals, Inc.
Figures
References
-
- Bleyer AJ, Russell GB, Satko SG. Sudden and cardiac death rates in hemodialysis patients. Kidney International. 1999;55:1553–1559. - PubMed
-
- Bleyer AJ, Hartman J, Brannon PC, Reeves-Daniel A, Satko SG, Russell G. Characteristics of sudden death in hemodialysis patients. Kidney International. 2006;69:2268–2273. - PubMed
-
- Karnik JA, Young BS, Lew NL, Herget M, Dubinsky C, Lazaraus JM, Chertow GM. Cardiac arrest and sudden death in dialysis units. Kidney Int. 2001;60:350–357. - PubMed
-
- Genovesi S, Valsecchi MG, Rossi E, Pogliani D, Acquistapace I. Sudden death and associated factors in a historical cohort of chronic hemodialysis patients. Nephrol Dial Transplant. 2009;24:2529–2536. - PubMed
-
- Foley RN, Gilbertson DT, Murray T, Collins AJ. Long interdialytic interval and mortality among patients receiving hemodialysis. NEJM. 2011;365(12):1099–1107. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
