

Optical control of focal epilepsy in vivo with caged γ-aminobutyric acid
- PMID: 22275253
- PMCID: PMC4133113
- DOI: 10.1002/ana.22596
Optical control of focal epilepsy in vivo with caged γ-aminobutyric acid
Abstract
Objective: There is enormous clinical potential in exploiting the spatial and temporal resolution of optical techniques to modulate pathophysiological neuronal activity, especially intractable focal epilepsy. We have recently utilized a new ruthenium-based caged compound, ruthenium-bipyridine-triphenylphosphine-γ-aminobutyric acid (RuBi-GABA), which releases GABA when exposed to blue light, to rapidly terminate paroxysmal activity in vitro and in vivo.
Methods: The convulsant 4-aminopyridine was used to induce interictal activity and seizures in rat neocortical slices and anesthetized rats. We examined the effect of blue light, generated by a small, light-emitting diode (LED), on the frequency and duration of ictal activity in the presence and absence of RuBi-GABA.
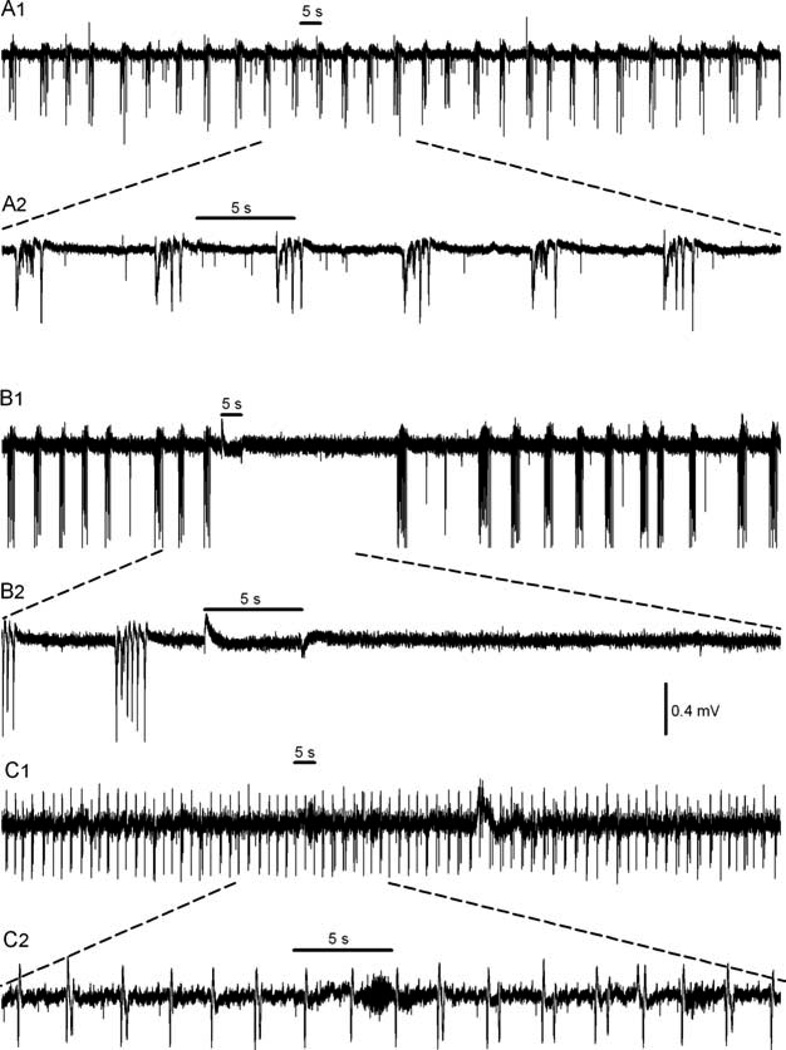
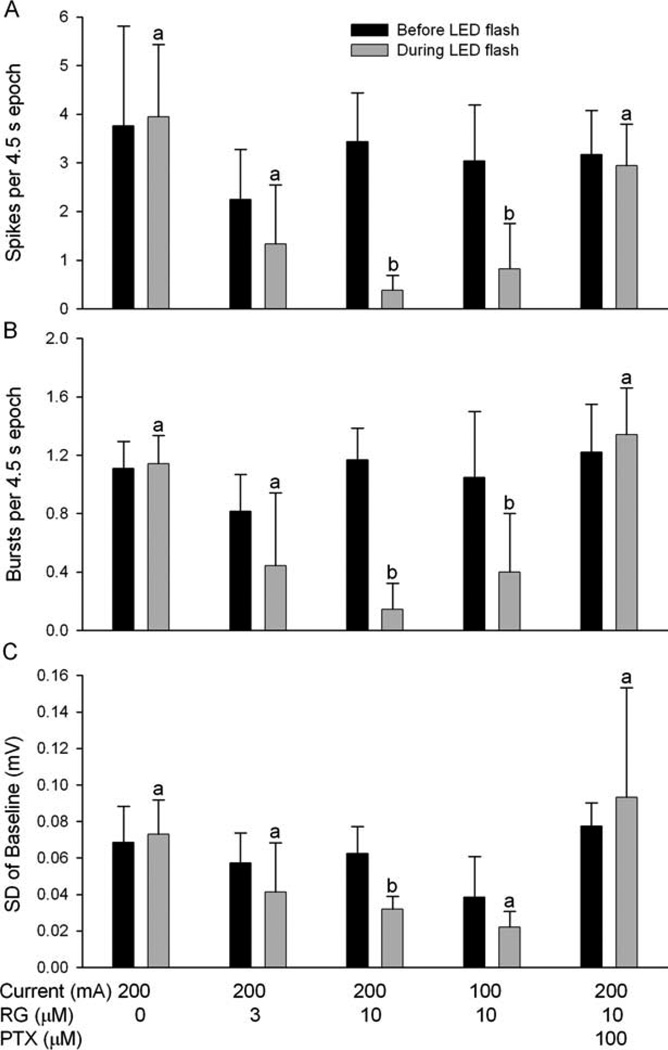
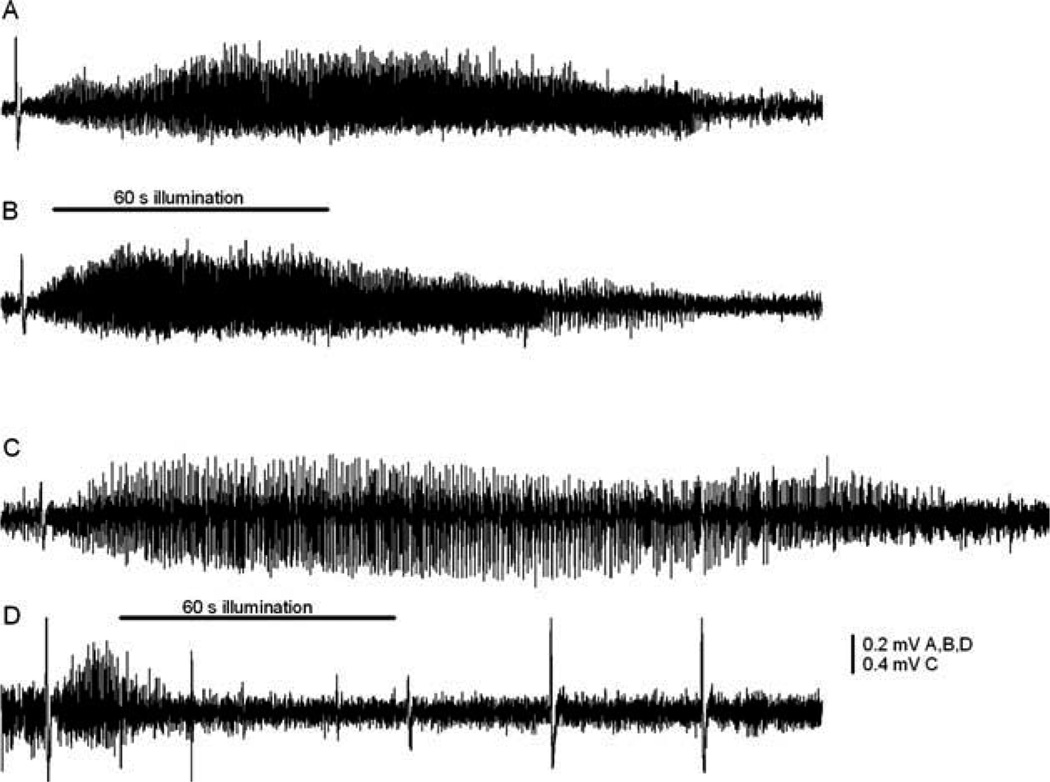
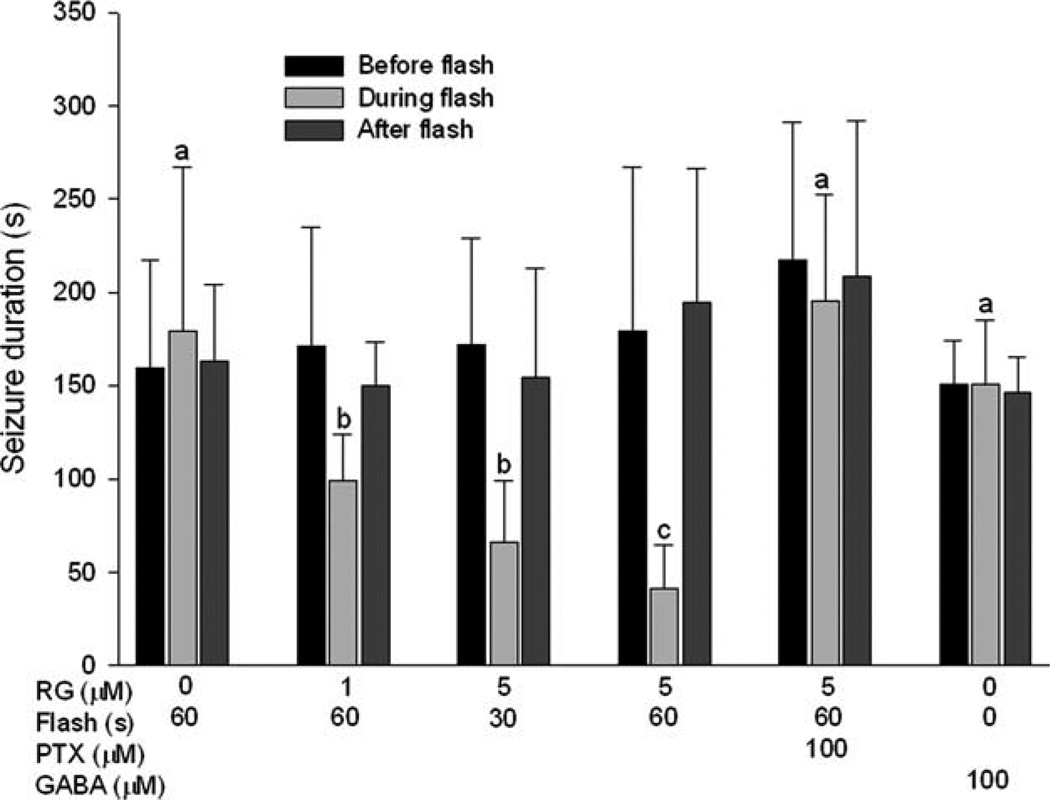
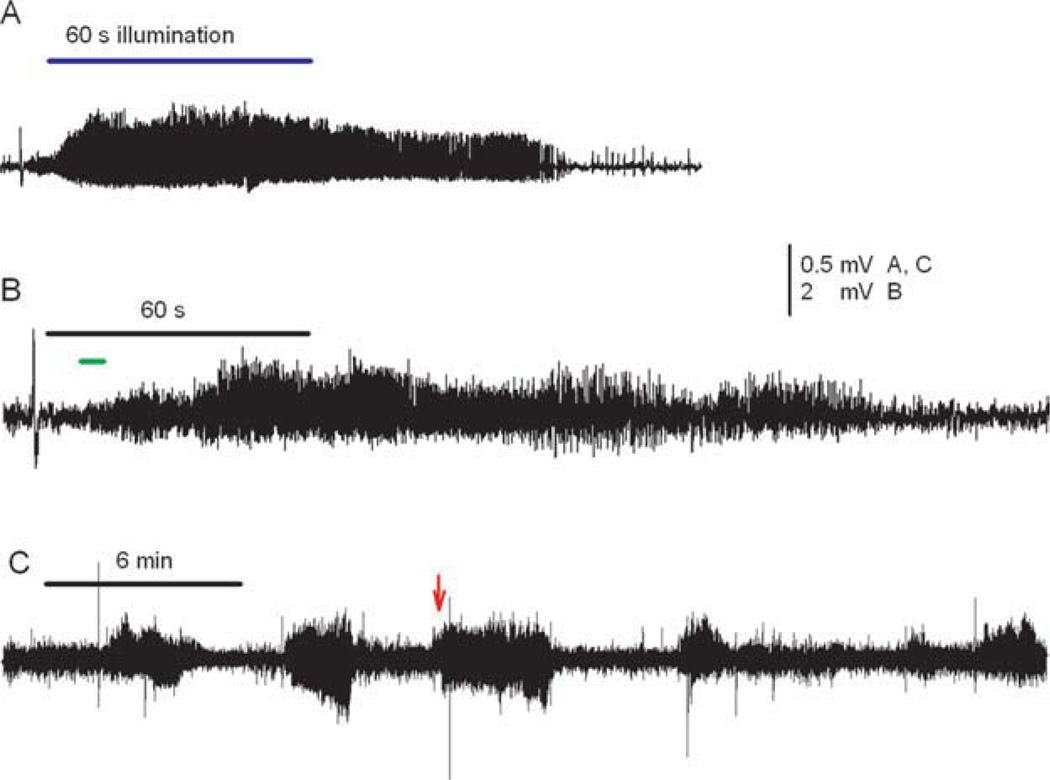
Results: Neither blue light alone, nor low concentrations of RuBi-GABA, affected interictal activity or baseline electrical activity in neocortical slices. However, brief, blue illumination of RuBi-GABA, using our LED, dramatically reduced extracellular spikes and bursts. More impressively, illumination of locally applied RuBi-GABA rapidly terminated in vivo seizures induced by topical application of 4-aminopyridine. The RuBi-GABA effect was blocked by the GABA(A) antagonist picrotoxin, but not duplicated by direct application of GABA.
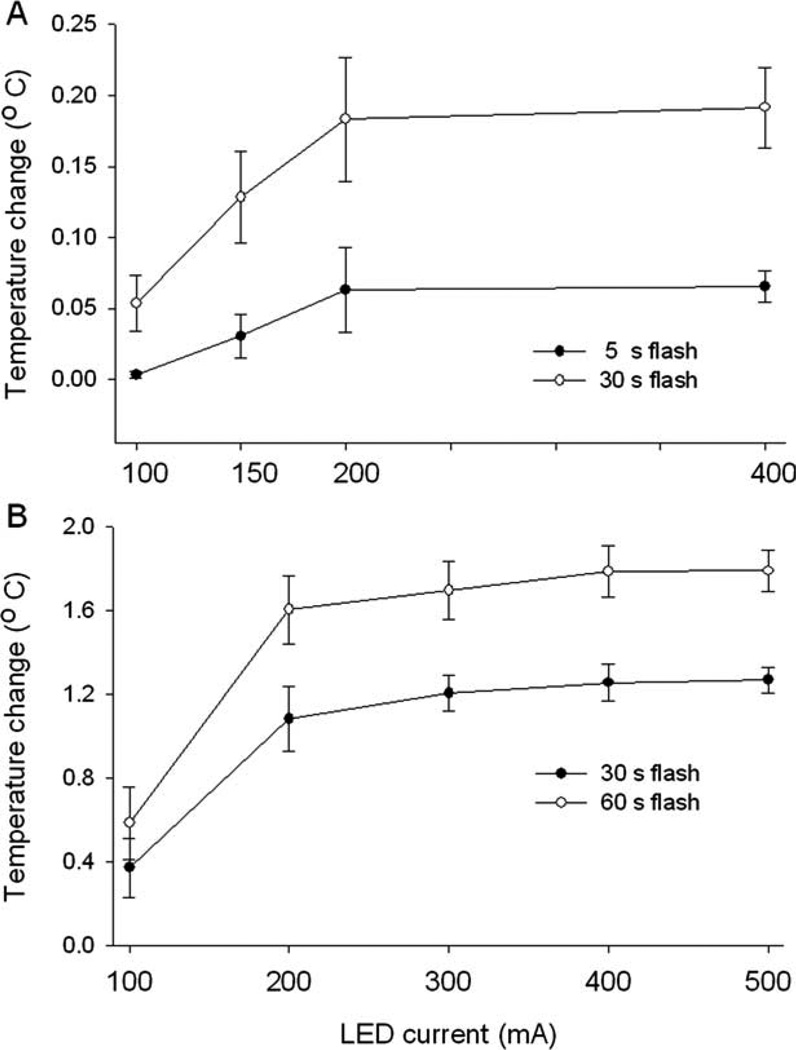
Interpretation: This is the first example of optical control of in vivo epilepsy, proving that there is sufficient cortical light penetration from an LED and diffusion of caged GABA to quickly terminate intense focal seizures. We are aware that many obstacles need to be overcome before this technique can be translated to patients, but at the moment, this represents a feasible method for harnessing optical techniques to fabricate an implantable device for the therapy of neocortical epilepsy.
Copyright © 2011 American Neurological Association.
Conflict of interest statement
R.Y.: employment, HHMI; patents, coinventor of RuBi-GABA but has received no royalties. S.M.R.: employment, University of Minnesota; grants/grants pending, NIH, CURE.
Figures
Similar articles
-
Photolysis of Caged-GABA Rapidly Terminates Seizures In Vivo: Concentration and Light Intensity Dependence.Front Neurol. 2017 May 18;8:215. doi: 10.3389/fneur.2017.00215. eCollection 2017. Front Neurol. 2017. PMID: 28572790 Free PMC article.
-
Recording of Neural Activity With Modulation of Photolysis of Caged Compounds Using Microelectrode Arrays in Rats With Seizures.IEEE Trans Biomed Eng. 2019 Nov;66(11):3080-3087. doi: 10.1109/TBME.2019.2900251. Epub 2019 Feb 20. IEEE Trans Biomed Eng. 2019. PMID: 30794501
-
Optical suppression of experimental seizures in rat brain slices.Epilepsia. 2010 Jan;51(1):127-35. doi: 10.1111/j.1528-1167.2009.02252.x. Epub 2009 Aug 8. Epilepsia. 2010. PMID: 19674053
-
Optical triggered seizures using a caged 4-Aminopyridine.Front Neurosci. 2015 Feb 4;9:25. doi: 10.3389/fnins.2015.00025. eCollection 2015. Front Neurosci. 2015. PMID: 25698919 Free PMC article.
-
The therapeutic potential of focal cooling for neocortical epilepsy.Neurotherapeutics. 2009 Apr;6(2):251-7. doi: 10.1016/j.nurt.2008.12.002. Neurotherapeutics. 2009. PMID: 19332317 Free PMC article. Review.
Cited by
-
Photopotentiation of the GABAA receptor with caged diazepam.Proc Natl Acad Sci U S A. 2019 Oct 15;116(42):21176-21184. doi: 10.1073/pnas.1902383116. Epub 2019 Oct 1. Proc Natl Acad Sci U S A. 2019. PMID: 31575739 Free PMC article.
-
Ex Vivo Feedback Control of Neurotransmission Using a Photocaged Adenosine A1 Receptor Agonist.Int J Mol Sci. 2022 Aug 10;23(16):8887. doi: 10.3390/ijms23168887. Int J Mol Sci. 2022. PMID: 36012151 Free PMC article.
-
Shining light on epilepsy: optical approaches for treating seizures.Epilepsy Curr. 2013 Mar;13(2):95-6. doi: 10.5698/1535-7597-13.2.95. Epilepsy Curr. 2013. PMID: 23646017 Free PMC article. No abstract available.
-
A Visible-Light-Sensitive Caged Serotonin.ACS Chem Neurosci. 2017 May 17;8(5):1036-1042. doi: 10.1021/acschemneuro.7b00083. Epub 2017 May 4. ACS Chem Neurosci. 2017. PMID: 28460173 Free PMC article.
-
Photolysis of Caged-GABA Rapidly Terminates Seizures In Vivo: Concentration and Light Intensity Dependence.Front Neurol. 2017 May 18;8:215. doi: 10.3389/fneur.2017.00215. eCollection 2017. Front Neurol. 2017. PMID: 28572790 Free PMC article.
References
-
- Sander J. The natural history of epilepsy in the era of new antiepileptic drugs and surgical treatment. Epilepsia. 2003;44(suppl 1):17–20. - PubMed
-
- Tellez-Zenteno J, Dhar R, Hernandez-Ronquillo L, et al. Long-term outcomes in epilepsy surgery: antiepileptic drugs, mortality, cognitive and psychosocial aspects. Brain. 2007;130:334–345. - PubMed
-
- Spencer S, Huh L. Outcomes of epilepsy surgery in adults and children. Lancet Neurol. 2008;7:525–537. - PubMed
-
- Fisher R, Salanova V, Witt T, et al. Electrical stimulation of the anterior nucleus of thalamus for treatment of refractory epilepsy. Epilepsia. 2010;51:899–908. - PubMed
-
- Eder H, Jones D, Fisher R. Local perfusion of diazepam attenuates interictal and ictal events in the bicuculline model of epilepsy in rats. Epilepsia. 1997;38:516–521. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
