

Prediction of adverse pregnancy outcome by the presence of lupus anticoagulant, but not anticardiolipin antibody, in patients with antiphospholipid antibodies
- PMID: 22275304
- PMCID: PMC3357451
- DOI: 10.1002/art.34402
Prediction of adverse pregnancy outcome by the presence of lupus anticoagulant, but not anticardiolipin antibody, in patients with antiphospholipid antibodies
Abstract
Objective: To investigate which serologic and clinical findings predict adverse pregnancy outcome in patients with antiphospholipid antibody (aPL) and to test the hypothesis that a pattern of clinical and serologic variables can identify women at highest risk of adverse pregnancy outcome.
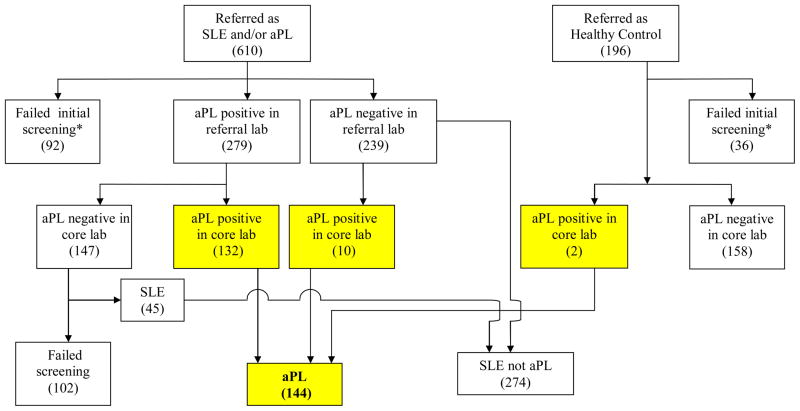
Methods: Women enrolled in a multicenter prospective observational study of risk factors for adverse pregnancy outcome in patients with aPL (lupus anticoagulant [LAC], anticardiolipin antibody [aCL], and/or antibody to β2-glycoprotein I [anti-β2 GPI]) and/or systemic lupus erythematosus (SLE) were recruited for the present prospective study. Demographic, clinical, serologic, and treatment data were recorded at the time of the first study visit. The relationship between individual and combined variables and adverse pregnancy outcome was assessed by bivariate and multivariate analysis.
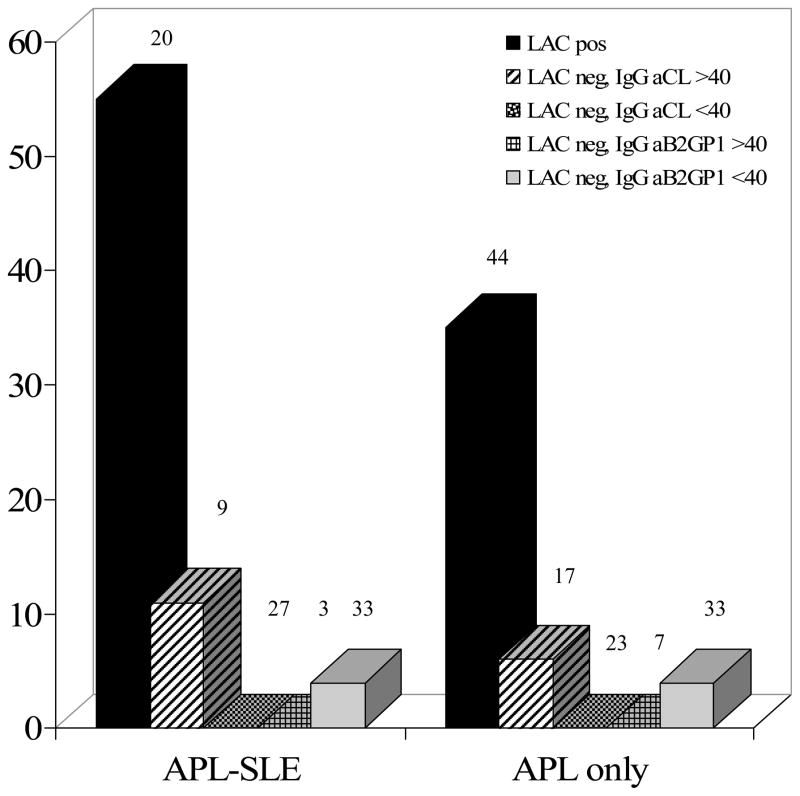
Results: Between 2003 and 2011 we enrolled 144 pregnant patients, of whom 28 had adverse pregnancy outcome. Thirty-nine percent of the patients with LAC had adverse pregnancy outcome, compared to 3% of those who did not have LAC (P<0.0001). Among women with IgG aCL at a level of ≥40 units/ml, only 8% of those who were LAC negative had adverse pregnancy outcome, compared to 43% of those who were LAC positive (P=0.002). IgM aCL, IgG anti-β2 GPI, and IgM anti-β2 GPI did not predict adverse pregnancy outcome. In bivariate analysis, adverse pregnancy outcome occurred in 52% of patients with and 13% of patients without prior thrombosis (P=0.00005), and in 23% with SLE versus 17% without SLE (not significant); SLE was a predictor in multivariate analysis. Prior pregnancy loss did not predict adverse pregnancy outcome. Simultaneous positivity for aCL, anti-β2 GPI, and LAC did not predict adverse pregnancy outcome better than did positivity for LAC alone.
Conclusion: LAC is the primary predictor of adverse pregnancy outcome after 12 weeks' gestation in aPL-associated pregnancies. Anticardiolipin antibody and anti-β2 GPI, if LAC is not also present, do not predict adverse pregnancy outcome.
Copyright © 2012 by the American College of Rheumatology.
Figures
References
-
- Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost. 2006;4:295–306. - PubMed
-
- Derksen RH, de Groot PG. The obstetric antiphospholipid syndrome. J Reprod Immunol. 2008;77:41–50. - PubMed
-
- Tincani A, Bazzani C, Zingarelli S, Lojacono A. Lupus and the antiphospholipid syndrome in pregnancy and obstetrics: clinical characteristics, diagnosis, pathogenesis, and treatment. Semin Thromb Hemost. 2008;34:267–73. - PubMed
-
- Ruffatti A, Calligaro A, Hoxha A, Trevisanuto D, Ruffatti AT, Gervasi MT, et al. Laboratory and clinical features of pregnant women with antiphospholipid syndrome and neonatal outcome. Arthritis Care Res. 2010;62:302–307. - PubMed
-
- Ruffatti A, Tonello M, Visentin MS, Bontadi A, Hoxha A, De Carolis S, et al. Risk factors for pregnancy failure in patients with anti-phospholipd syndrome treated with conventional therapies: a multicentre, case-control study. Rheumatology. 2011;50:1684–1689. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
