

Diffuse pulmonary uptake on FDG-PET with normal CT diagnosed as intravascular large B-cell lymphoma: a case report and a discussion of the causes of diffuse FDG uptake in the lungs
- PMID: 22275725
- PMCID: PMC3266578
- DOI: 10.1102/1470-7330.2012.0002
Diffuse pulmonary uptake on FDG-PET with normal CT diagnosed as intravascular large B-cell lymphoma: a case report and a discussion of the causes of diffuse FDG uptake in the lungs
Abstract
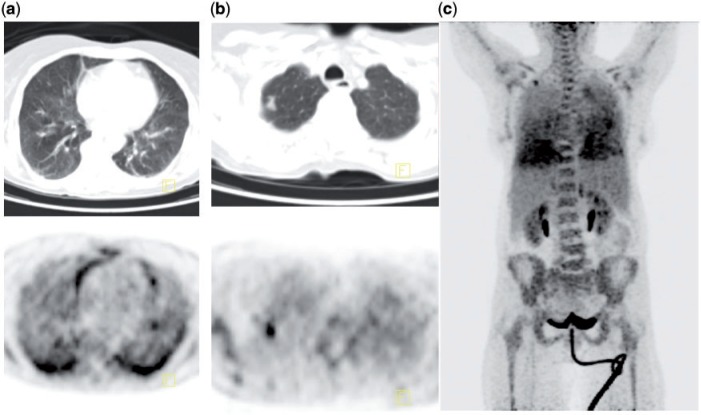
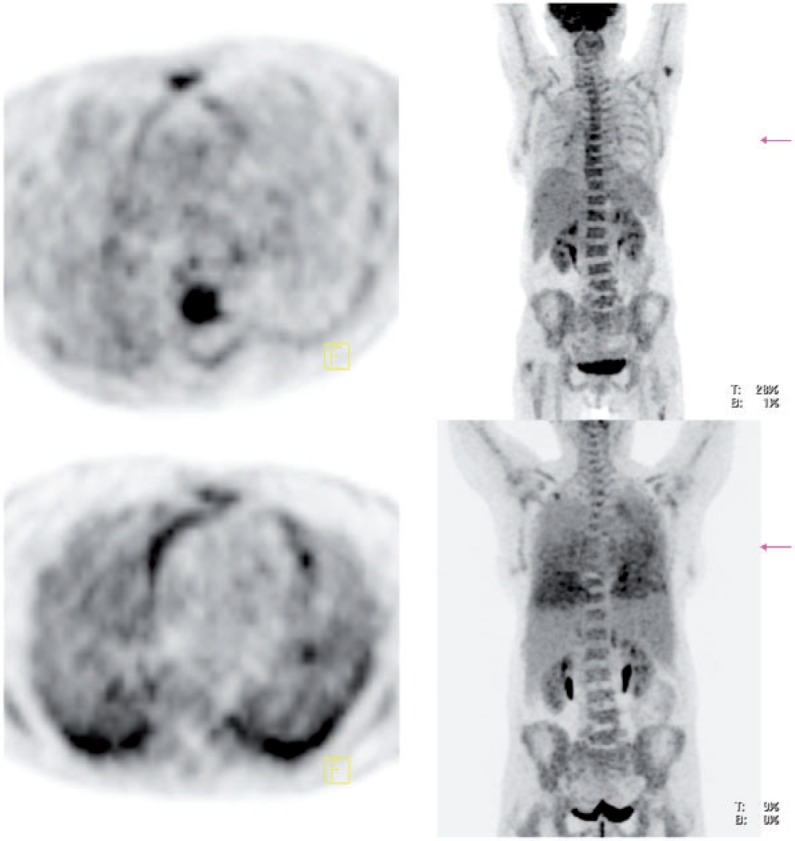
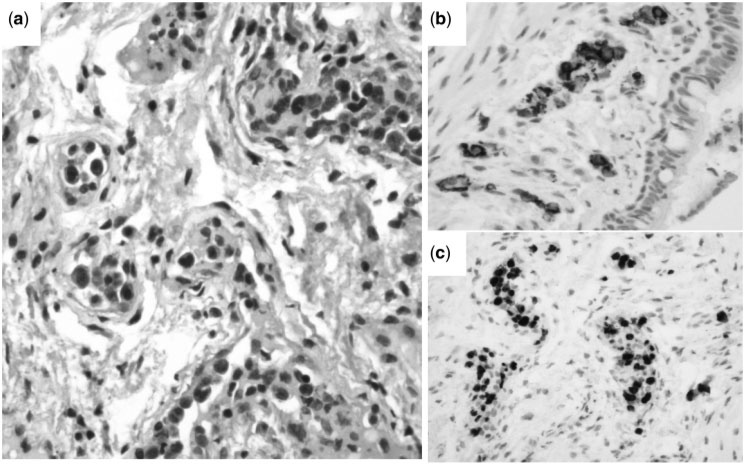
A 71-year-old woman was admitted to our hospital with asthenia, weight loss, fever, cognitive impairment and shortness of breath. Physical examination showed hemiparesis and cerebellar ataxia. There was no superficial lymphadenopathy. Blood tests showed raised levels of C-reactive protein and lactate dehydrogenase. Bone marrow aspiration and biopsy were negative. [18F]fluorodeoxyglucose (FDG)-positron emission tomography (PET)/computed tomography (CT) showed intense uptake within a right apical nodule and intense and diffuse uptake of FDG in the lungs without corresponding structural CT abnormality. Lung biopsy showed intravascular large B-cell lymphoma (IVLBCL). FDG-PET findings in IVLBCL and causes of diffuse FDG lung uptake with and without CT abnormalities are discussed.
Figures

Similar articles
-
Prognostic Importance of Bone Marrow Uptake on Baseline 18F-FDG Positron Emission Tomography in Diffuse Large B Cell Lymphoma.Cancer Biother Radiopharm. 2016 Dec;31(10):361-365. doi: 10.1089/cbr.2016.2132. Cancer Biother Radiopharm. 2016. PMID: 27996313
-
Normal blood glucose level and (18)F-FDG PET/CT.Rev Esp Med Nucl Imagen Mol. 2012 Jul-Aug;31(4):210-2. doi: 10.1016/j.remn.2012.01.008. Epub 2012 Apr 6. Rev Esp Med Nucl Imagen Mol. 2012. PMID: 22980129
-
Intravascular large B-cell lymphoma diagnosed by FDG-PET/CT and endometrial biopsy.Rinsho Ketsueki. 2011 Nov;52(11):1777-81. Rinsho Ketsueki. 2011. PMID: 22185801
-
FDG-PET/CT is a pivotal imaging modality to diagnose rare intravascular large B-cell lymphoma: case report and review of literature.Hematol Oncol. 2015 Jun;33(2):99-109. doi: 10.1002/hon.2140. Epub 2014 May 21. Hematol Oncol. 2015. PMID: 24850057 Review.
-
18F-FDG-PET/CT in lymphoma: two decades of experience.Rev Esp Med Nucl Imagen Mol. 2012 Nov-Dec;31(6):340-9. doi: 10.1016/j.remn.2012.06.001. Epub 2012 Jul 26. Rev Esp Med Nucl Imagen Mol. 2012. PMID: 22841459 Review. English, Spanish.
Cited by
-
Early detection of intravascular large B-cell lymphoma by (18)FDG-PET/CT with diffuse FDG uptake in the lung without respiratory symptoms or chest CT abnormalities.Asia Ocean J Nucl Med Biol. 2014 Spring;2(1):65-8. Asia Ocean J Nucl Med Biol. 2014. PMID: 27408860 Free PMC article.
-
Primary pulmonary intravascular large B-cell lymphoma: A report of three cases and literature review.Oncol Lett. 2018 Mar;15(3):3610-3613. doi: 10.3892/ol.2018.7753. Epub 2018 Jan 9. Oncol Lett. 2018. PMID: 29467882 Free PMC article.
-
Intravascular large B-cell lymphoma with hemophagocytic syndrome (Asian variant) in a Caucasian patient.Int J Clin Exp Pathol. 2012;5(5):448-54. Epub 2012 May 23. Int J Clin Exp Pathol. 2012. PMID: 22808298 Free PMC article.
-
EBV-positive intravascular large B-cell lymphoma of the liver: a case report and literature review.Diagn Pathol. 2020 Jun 8;15(1):72. doi: 10.1186/s13000-020-00989-x. Diagn Pathol. 2020. PMID: 32513269 Free PMC article. Review.
-
Intravascular large B-cell lymphoma manifesting as cholecystitis: report of an Asian variant showing gain of chromosome 18 with concurrent deletion of chromosome 6q.Int J Clin Exp Pathol. 2014 Oct 15;7(11):8181-9. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25550870 Free PMC article.
References
-
- Pfleger L, Tappeiner J. [On the recognition of systematized endotheliomatosis of the cutaneous blood vessels (reticuloendotheliosis?] Hautarzt. 1959;10:359–63. - PubMed
-
- Pontier S, Selves J, Escamilla R, Hermant C, Krempf M. [Intra-vascular lymphoma presenting with respiratory symptoms] Rev Mal Respir. 2003;20:782–5. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Research Materials