

doi: 10.3332/ecancer.2010.164.
Epub 2010 Feb 3.
The role of funding and policies on innovation in cancer drug development
Affiliations
- PMID: 22276026
- PMCID: PMC3234026
- DOI: 10.3332/ecancer.2010.164
Item in Clipboard
The role of funding and policies on innovation in cancer drug development
Ecancermedicalscience.
2010.
No abstract available
Figures
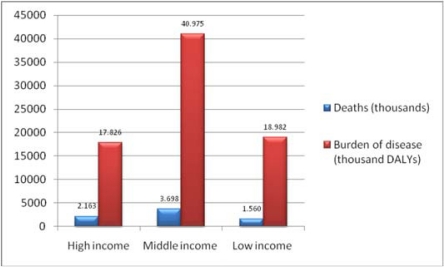
Source: [4].
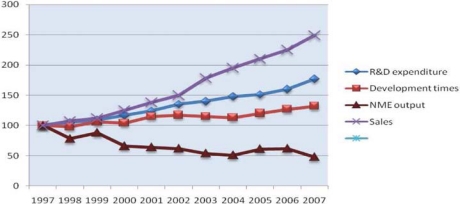
Global R&D expenditure, development times, NME output and global pharmaceutical sales (1997–2007) Notes: Each trend line has been indexed to 1997 values Development time data point for 2007 includes data from 2006 and 2007 only Source: CMR International and IMS Health
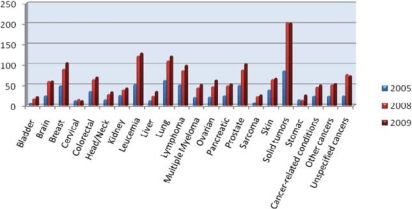
Number of new cancer drugs in development by type of cancer. Note: Some drugs are listed in more than one category. Source: PhRMA (‘New medicines in development for cancer’).
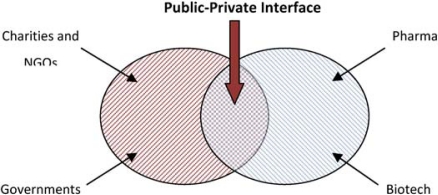
The public-private interface in cancer drug research and development. Source: The authors.
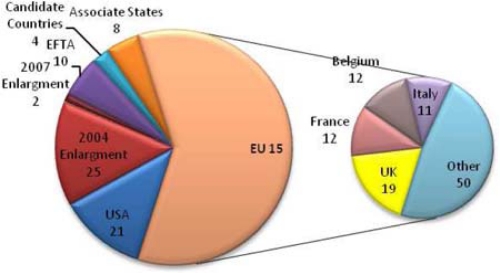
Number of public sector funding organisations by country. Source: The authors.
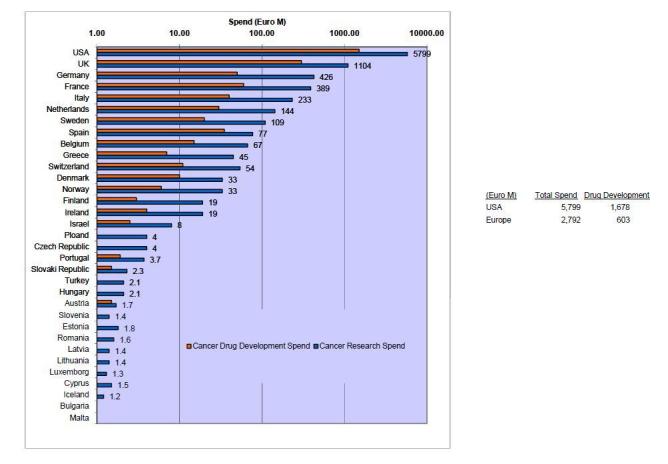
Direct cancer drug R&D (Spending on log scale). Source: The authors.
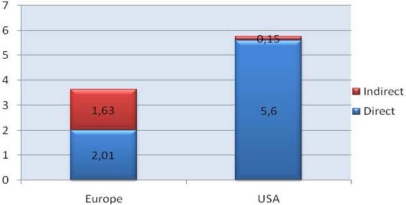
Estimated indirect cancer R&D funding.
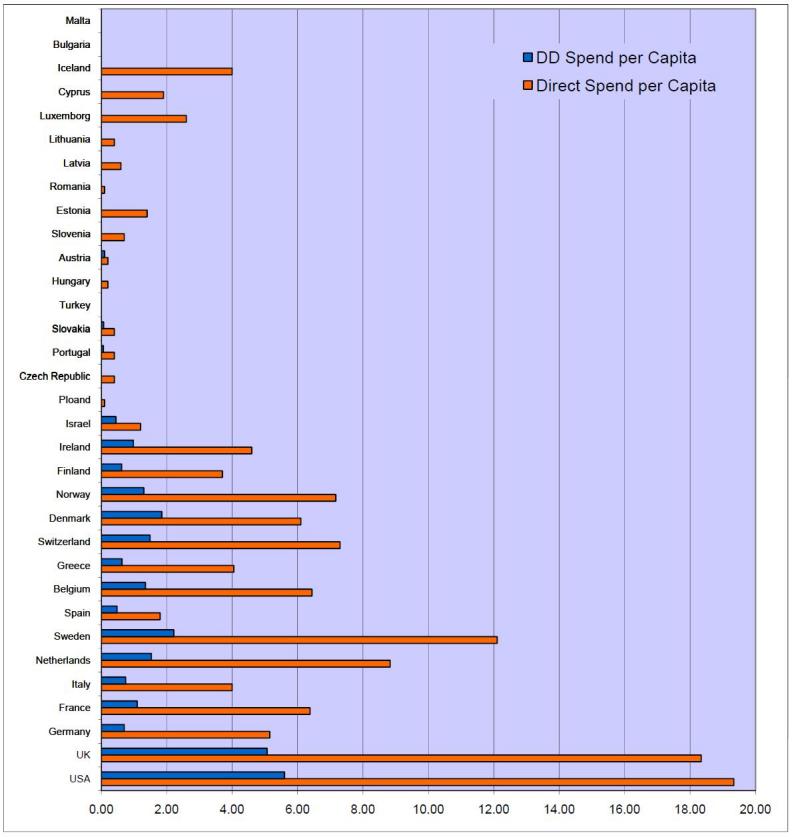
Cancer R&D direct spending (€) per capita. Source: The authors.
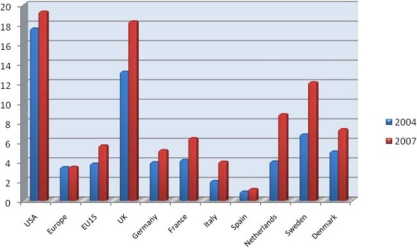
Direct cancer R&D spending per capita, 2004 versus 2007 (€). Source: ECRM (2004 data) and the Authors (2007 data).
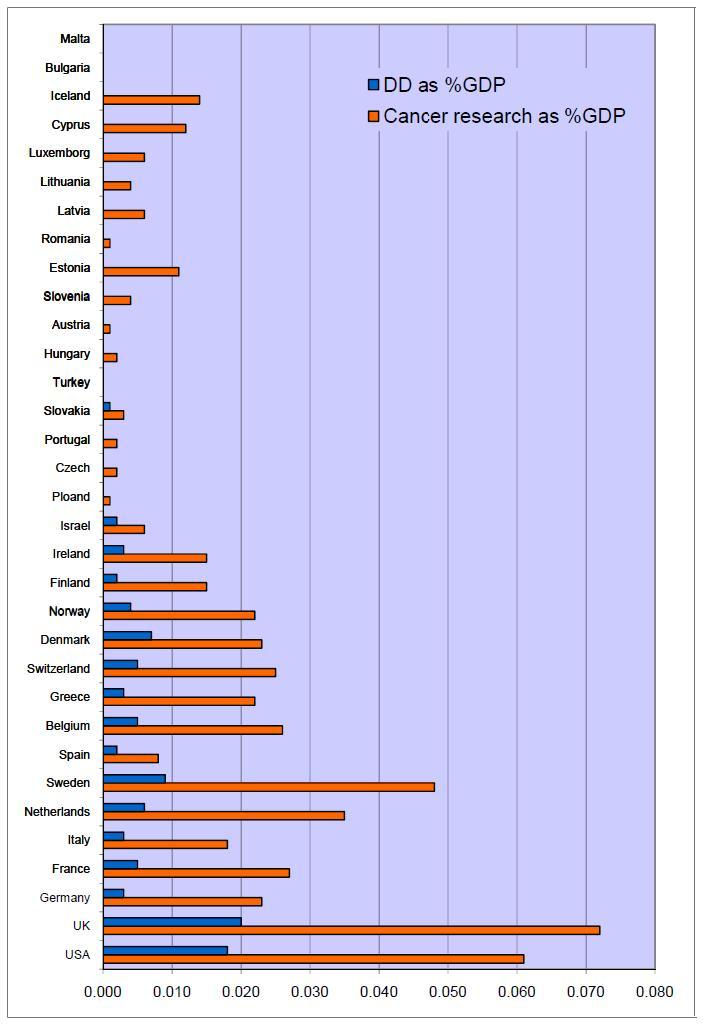
Cancer drug R&D and cancer R&D direct spending, % of GDP. Source: The authors.
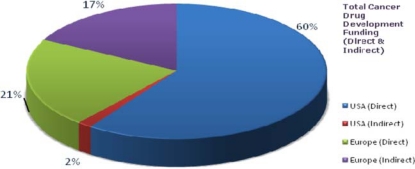
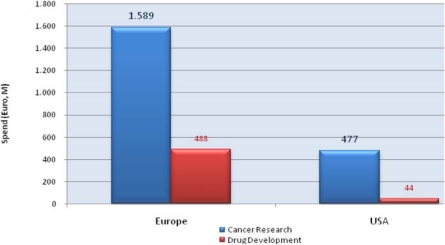
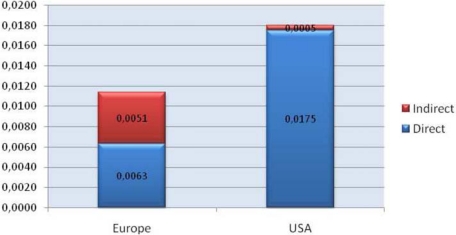
Route of cancer drug R&D funding. Source: The authors.
Cancer drug R&D spend per capita (€). Source: The authors.
Cancer drug R&D spend, % of GDP. Source: The authors.
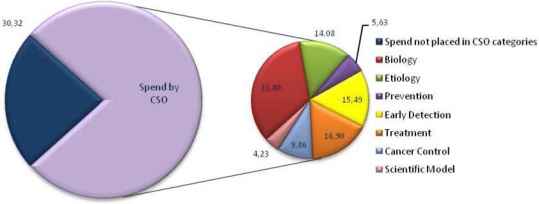
European cancer R&D spend by CSO category. Source: The authors.
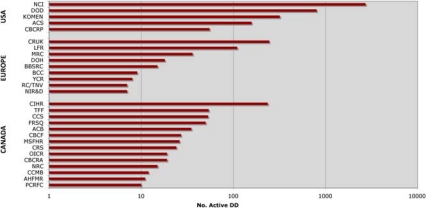
Number of active cancer drug development projects by funder, grouped by country (log scale). Source: The authors.
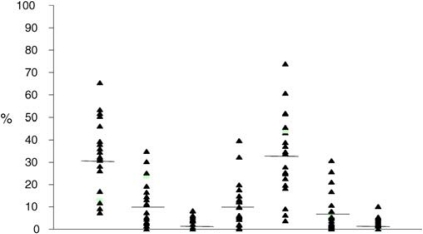
Scatter plot showing percentage of spend according to domain of research (by CSO category) for a sample of European Cancer Centres (n= 20). Source: The authors.
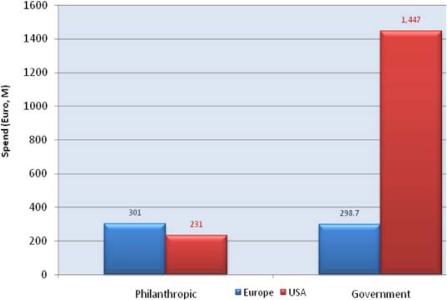
Drug R&D funding by charities and government (2007). Source: The authors.
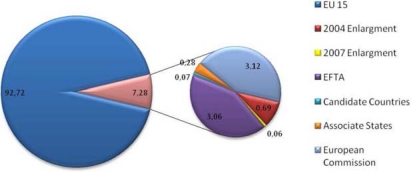
Percent of direct spend by political group in Europe (2007). Source: The authors.
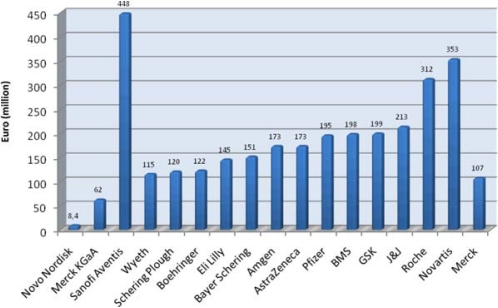
Private cancer drug development spend: major pharmaceutical companies (2004/ Phase III)* Note: *The figure does not include all industry (e.g. SME and biotechnology). Source: [7].
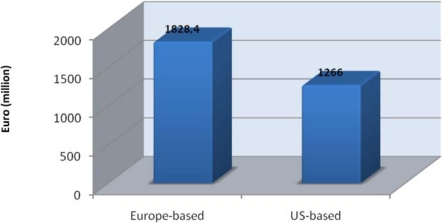
Private cancer R&D funding by company origin. Source: The authors.
Cancer drug development projects with joint private-public funding (%) (2007–2008). Source: The authors.
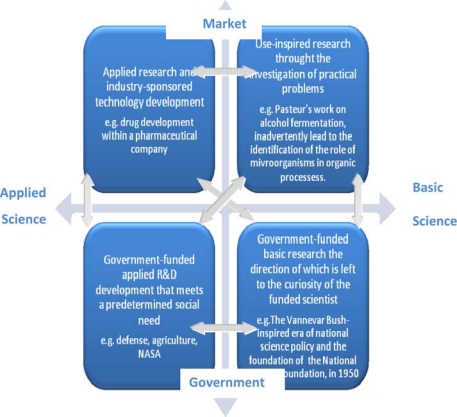
Interaction between basic versus applied science and between market versus government. Source: Adapted from [].
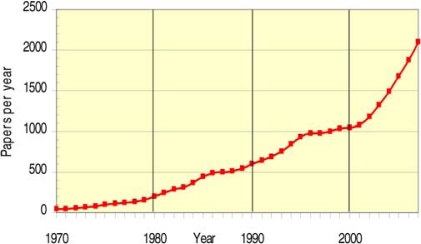
Total WoS output for 19 cancer drug research papers (3-year running means) (1970–2007)
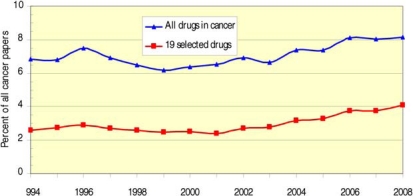
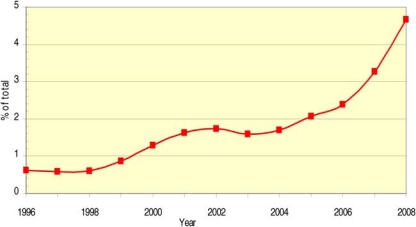
Proportion of total drug (blue) and 19 drugs (red) cancer research papers of total cancer research papers
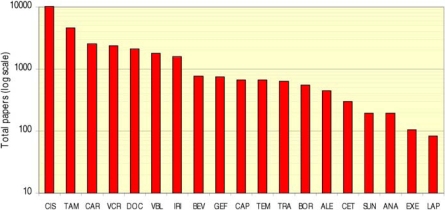
WoS cancer drug papers for 19 cancer drugs (1963–2009)
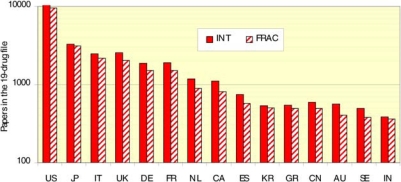
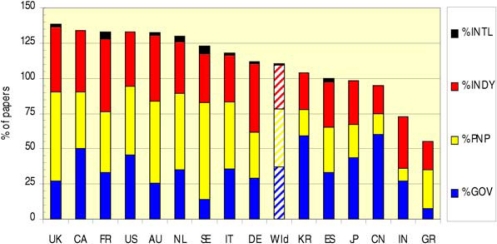
Distribution of papers in 15 countries (integer, fractional counts)
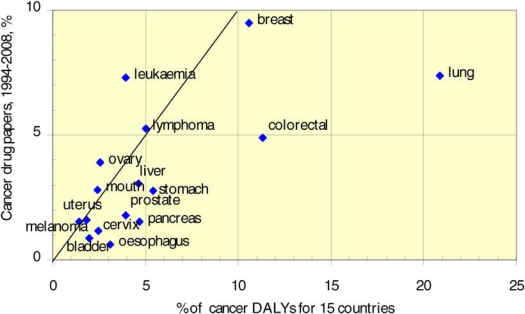
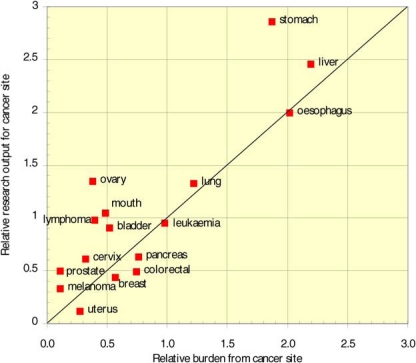
Cancer drug paper outputs (1994–2008) versus cancer burden of disease (% DALYs) (2004) (weighted by the countries’ presence in cancer drug research)
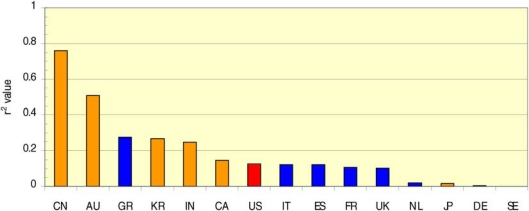
Country-specific correlation coefficient of cancer drug paper outputs versus burden for 16 cancer sites
China: cancer drug research output versus burden from 16 cancer sites
Mean research level (RL) of all cancer drug papers in five quintiles
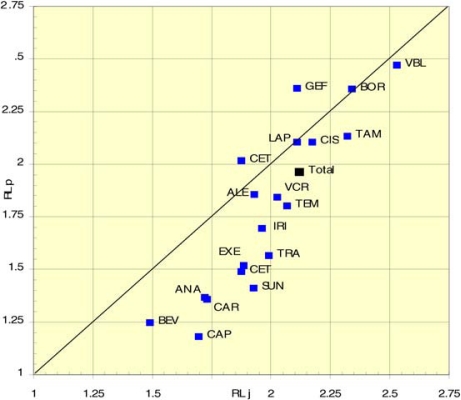
Mean research level (RL): journal source (RLj) versus title source (RLp) in 19 cancer drug papers (1963–2009)
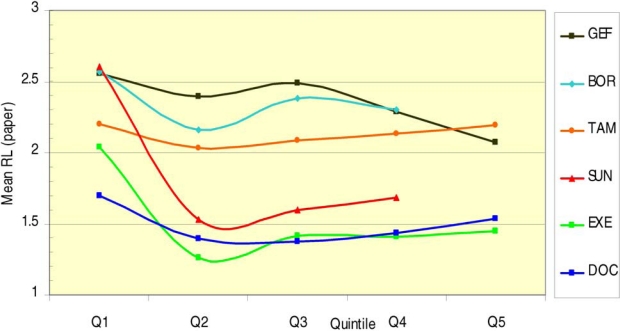
Average research level (RL) per time quintile for 6 cancer drugs
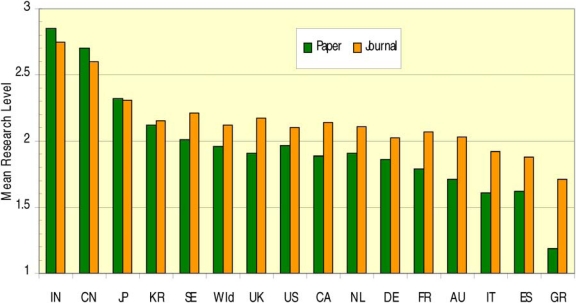
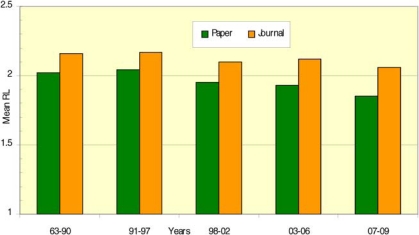
Mean research level (RL) from 15 countries in 19 cancer drug research papers per paper title (paper) and per journal source (journal)
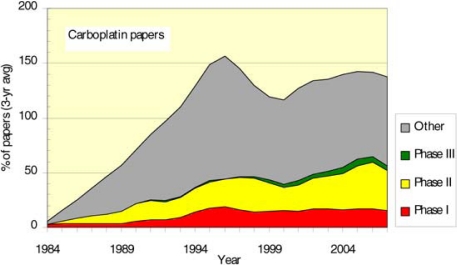
Phased carboplatin clinical trials longitudinal paper outputs (3-year running means)
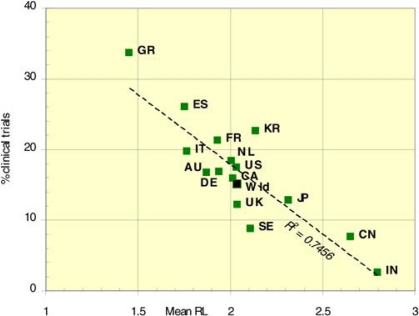
Percentage cancer drug clinical trials output per mean research level in 15 countries
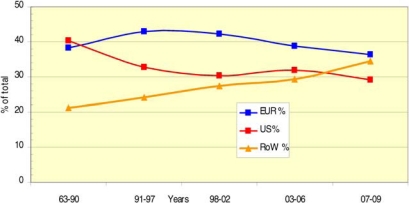
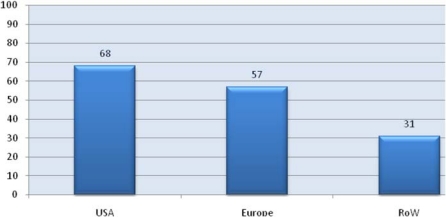
Geographical distribution of cancer drug papers in three world regions (USA, EUR 30, RoW) (quintiles, fractional counts) (1963–2009)
Chinese cancer drug papers, 3-year running means (fractional counts) (1996–2008)
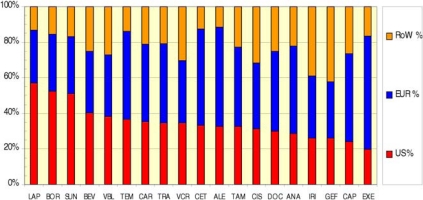
Distribution of 19 cancer drug papers by geographical region: USA, EUR30 and RoW (fractional counts)
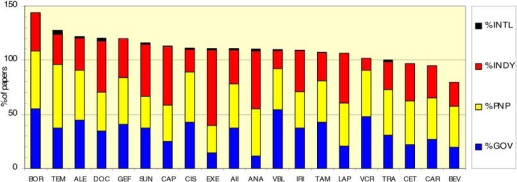
Funding sources in 19 cancer drug papers (1963–2009)
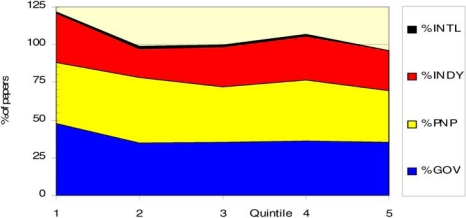
Funding sources for 6 out of 19 cancer drugs* in different time quintiles *Six drugs = carboplatin, cisplatin, docetaxel, irinotecan, tamoxifen and vincristine.
Funding sources for cancer drug papers in 15 leading countries (1963–2009)
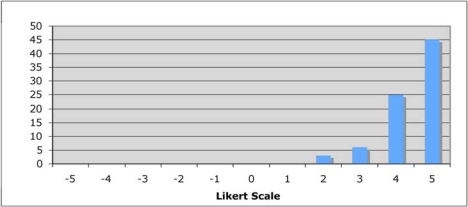
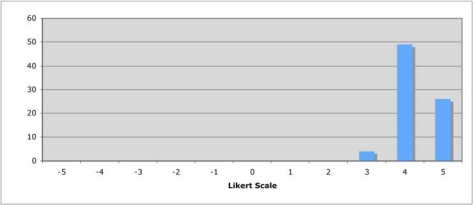
Is private sector support for drug development essential?
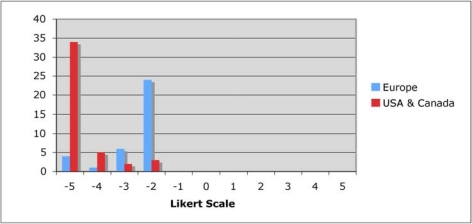
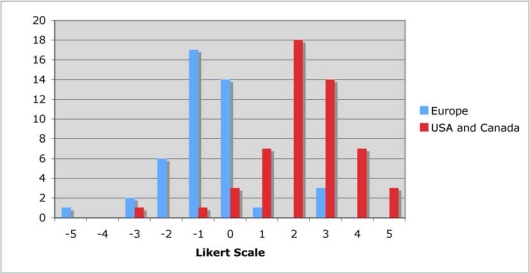
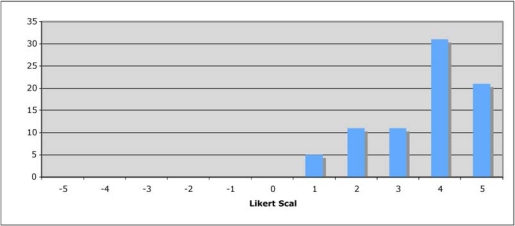
Is the current level of national public sector investment adequate?
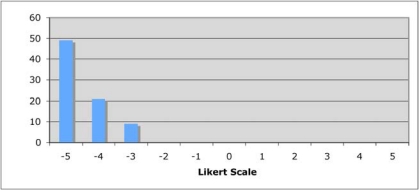
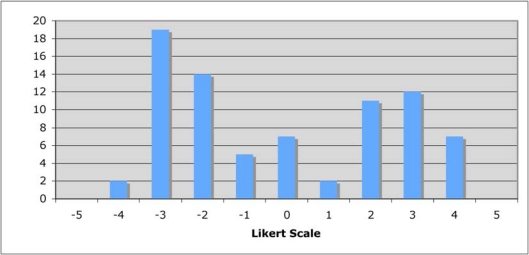
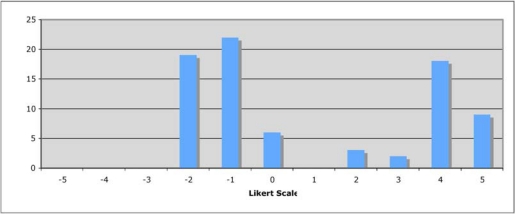
Does the public sector have a limited role in cancer drug development?
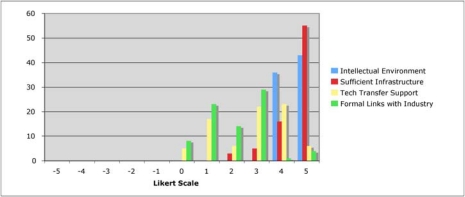
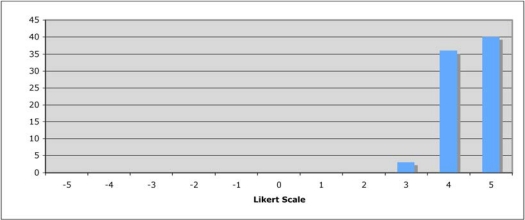
How important is the intellectual (academic faculty) environment?
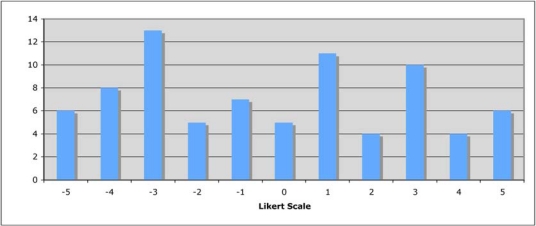
Are financial incentives important for public-private partnerships?
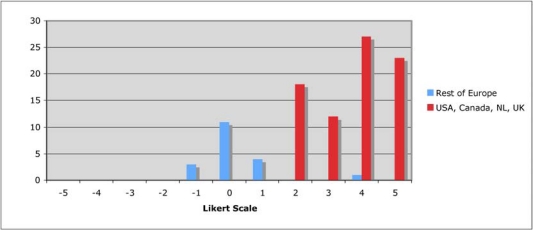
Should private sector support be short-term project based?
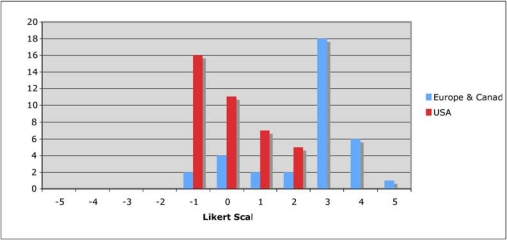
Should nationalisation of parts of the drug development process be considered?
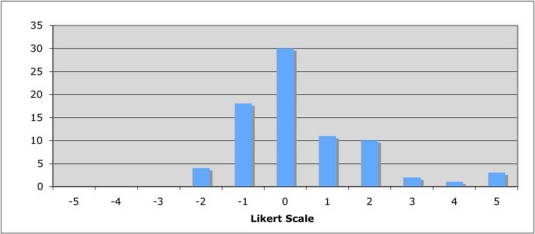
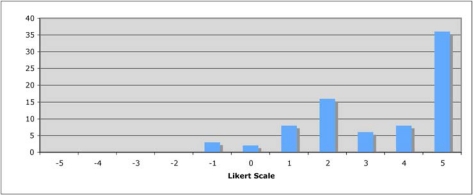
Is the balance between private and public cancer drug development correct?
Is the regulatory environment a key area for success?
How important are policies around the reimbursement of new cancer drugs to future success?
How important are supra-national funding initiatives?
How important are national funding policies from research funding organisations?
Is institutional support important for success in cancer drug discovery?
Are technology transfer and/or incentive schemes important policy areas?
Are new models in PPP are needed?
New models for R&D in cancer drug discovery and development are needed.
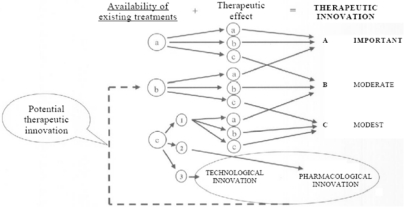
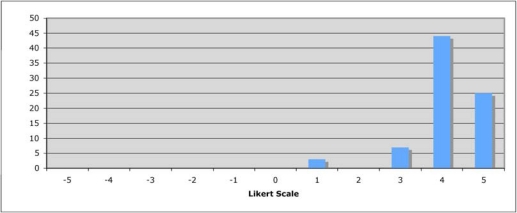
Assessing therapeutic innovation in Italy
References
-
- American Cancer Society Cancer Facts and Figures 2009.
-
- Kanavos P. The rising burden of cancer in the developing world. Annals Oncol. 2006;17(S8):viii16–23. - PubMed
-
- World Health Organisation . The Global Burden of Disease: 2004 update. WHO; 2008.
-
- Boyle P, Levin B, editors. World Cancer Report 2008. Lyon: International Agency for Research on Cancer; 2008.
LinkOut - more resources
Full Text Sources