

A single nucleotide polymorphism of the cholecystokinin-B receptor predicts risk for pancreatic cancer
- PMID: 22277584
- PMCID: PMC3336072
- DOI: 10.4161/cbt.13.3.18698
A single nucleotide polymorphism of the cholecystokinin-B receptor predicts risk for pancreatic cancer
Abstract
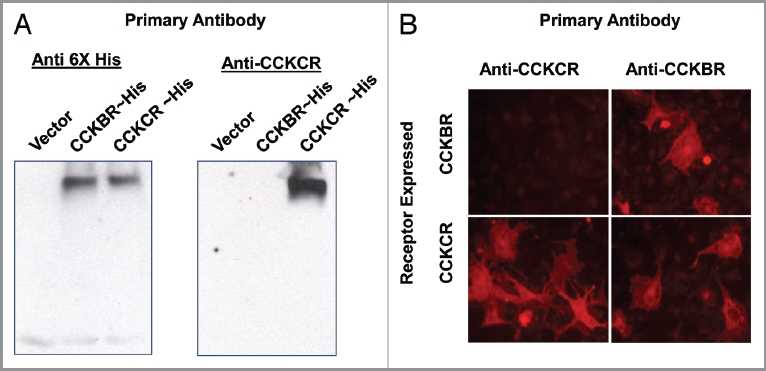
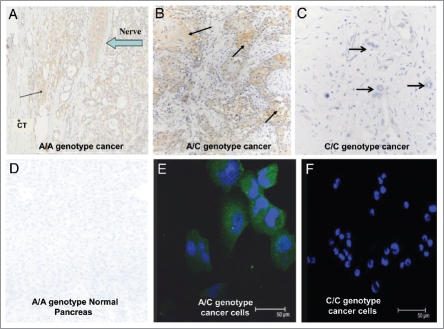
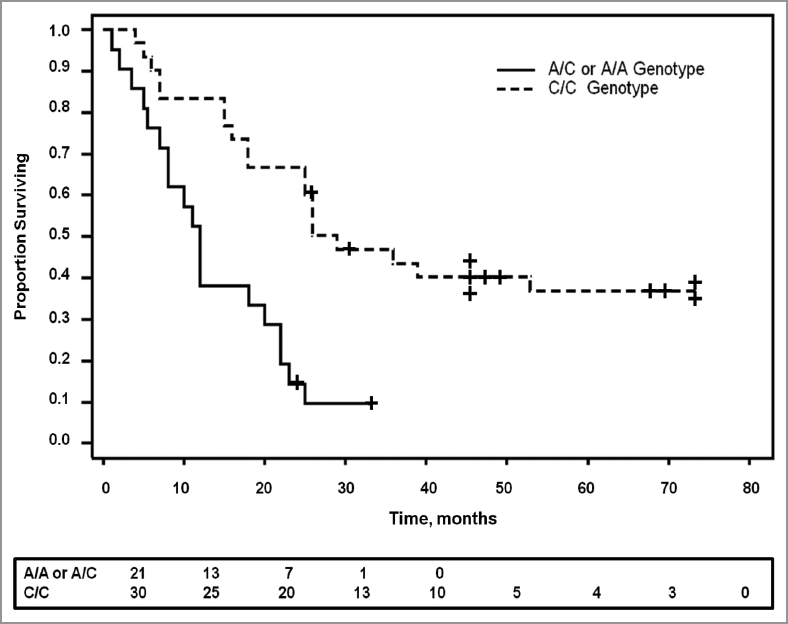
There currently are no tests available for early diagnosis or for the identification of patients at risk for development of pancreatic cancer. We report the discovery of single nucleotide polymorphism (SNP) in the cholecystokinin B receptor (CCKBR) gene predicts survival and risk of pancreatic cancer. Growth of human pancreatic cancer is stimulated by gastrin through the CCKBR and an alternatively spliced isoform of the CCKBR gene called CCKCR. One hundred and ten surgically resected benign and malignant pancreatic tissues as well as normal pancreas were prospectively evaluated for CCKBR genotype and protein expression. Analysis demonstrated the expression of the spliced isoform, CCKCR, was associated with a (SNP) (C > A) at position 32 of the intron 4 (IVS 4) of the CCKBR gene. Since the SNP is within an intron, it has not previously been identified in the GWAS studies. Only patients with the A/A or A/C genotypes, exhibited immunoreactivity to a selective CCKCR antibody. Survival among pancreatic cancer patients with the A-SNP was significantly shorter (p = 0.0001, hazard ratio = 3.63) compared with individuals with C/C genotype. Other variables such as surgical margins, lymph node status, histologic grade or adjuvant chemotherapy were not associated with survival. Furthermore, having one or two of the A-alleles was found to increase the risk of pancreatic adenocarcinoma by 174% (p = 0.0192) compared with the C/C wild type. Cancer cells transfected to overexpress the CCKCR demonstrated increased proliferation over controls. Genetic screening for this SNP may aid in early detection of pancreatic cancer in high risk subjects.
Figures

Similar articles
-
Distribution of cholecystokinin-B receptor genotype between patients with pancreatic cancer and controls and its impact on survival.Pancreas. 2015 Mar;44(2):236-42. doi: 10.1097/MPA.0000000000000263. Pancreas. 2015. PMID: 25469546 Free PMC article.
-
A Common CCK-B Receptor Intronic Variant in Pancreatic Adenocarcinoma in a Hungarian Cohort.Pancreas. 2016 Apr;45(4):541-5. doi: 10.1097/MPA.0000000000000539. Pancreas. 2016. PMID: 26646278 Free PMC article.
-
Impact of TP53 codon 72 and MDM2 SNP 309 polymorphisms in pancreatic ductal adenocarcinoma.PLoS One. 2015 Mar 3;10(3):e0118829. doi: 10.1371/journal.pone.0118829. eCollection 2015. PLoS One. 2015. PMID: 25734904 Free PMC article.
-
A Cholecystokinin B Receptor-Specific DNA Aptamer for Targeting Pancreatic Ductal Adenocarcinoma.Nucleic Acid Ther. 2017 Feb;27(1):23-35. doi: 10.1089/nat.2016.0621. Epub 2016 Oct 18. Nucleic Acid Ther. 2017. PMID: 27754762 Free PMC article.
-
What are the pancreatic target cells for gastrin and its CCKB receptor? Is this a couple for cancerous cells?Med Sci Monit. 2004 Oct;10(10):RA242-6. Epub 2004 Sep 23. Med Sci Monit. 2004. PMID: 15448615 Review.
Cited by
-
Distribution of cholecystokinin-B receptor genotype between patients with pancreatic cancer and controls and its impact on survival.Pancreas. 2015 Mar;44(2):236-42. doi: 10.1097/MPA.0000000000000263. Pancreas. 2015. PMID: 25469546 Free PMC article.
-
Genetic variants of the peroxisome proliferator-activated receptor (PPAR) signaling pathway genes and risk of pancreatic cancer.Mol Carcinog. 2020 Aug;59(8):930-939. doi: 10.1002/mc.23208. Epub 2020 May 5. Mol Carcinog. 2020. PMID: 32367578 Free PMC article.
-
Germline Mutation of the CCK Receptor: A Novel Biomarker for Pancreas Cancer.Clin Transl Gastroenterol. 2016 Jan 7;7(1):e134. doi: 10.1038/ctg.2015.61. Clin Transl Gastroenterol. 2016. PMID: 26741064 Free PMC article.
-
Novel strategies for managing pancreatic cancer.World J Gastroenterol. 2014 Oct 28;20(40):14717-25. doi: 10.3748/wjg.v20.i40.14717. World J Gastroenterol. 2014. PMID: 25356034 Free PMC article. Review.
-
Cholecystokinin receptor antagonist alters pancreatic cancer microenvironment and increases efficacy of immune checkpoint antibody therapy in mice.Cancer Immunol Immunother. 2018 Feb;67(2):195-207. doi: 10.1007/s00262-017-2077-9. Epub 2017 Oct 17. Cancer Immunol Immunother. 2018. PMID: 29043413 Free PMC article.
References
-
- Wolff RA. Novel therapies for pancreatic cancer. Cancer J. 2001;7:349–258. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical