

The natural history of preclinical diastolic dysfunction: a population-based study
- PMID: 22278404
- PMCID: PMC3555563
- DOI: 10.1161/CIRCHEARTFAILURE.110.959668
The natural history of preclinical diastolic dysfunction: a population-based study
Abstract
Background: Preclinical diastolic dysfunction (PDD) has been broadly defined as subjects with left ventricular diastolic dysfunction, without the diagnosis of congestive heart failure (HF) and with normal systolic function. Our objective was to determine the risk factors associated with the progression from PDD (stage B) HF to symptomatic (stage C) HF.
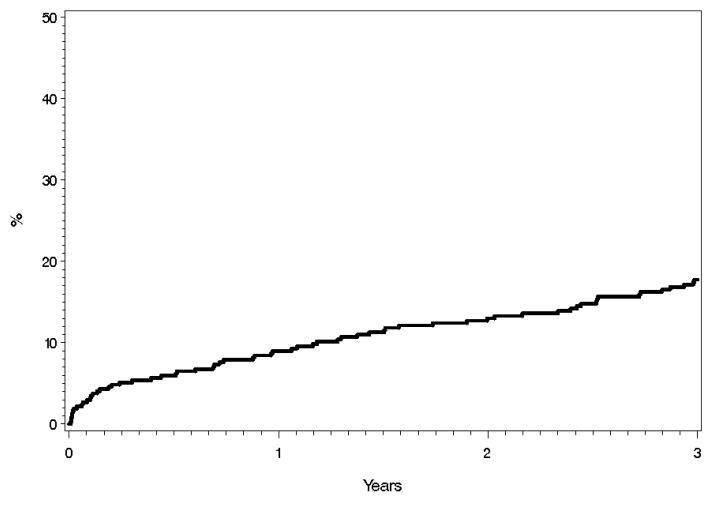
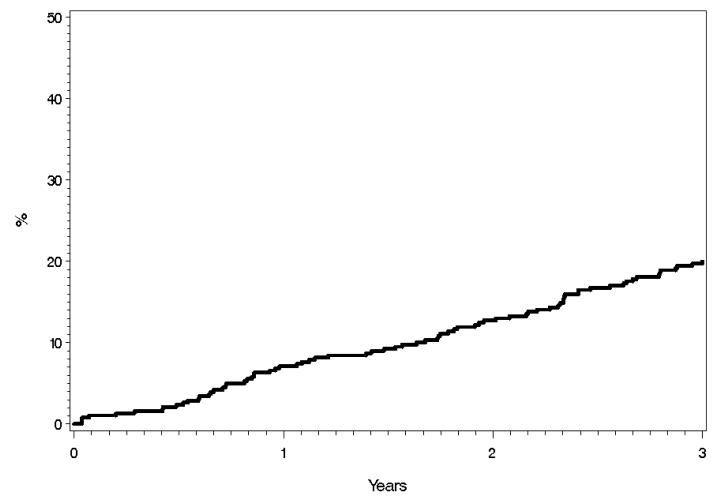
Methods and results: Using the resources of the Rochester Epidemiology Project, all residents of Olmsted County, MN, who underwent echocardiography between January 1, 2004, and December 31, 2005, and had grade 2-4 diastolic dysfunction and ejection fraction ≥50% were identified. Patients with a diagnosis of HF before or within 30 days of the echocardiogram were excluded. Patients were also excluded if they had a diagnosis of atrial fibrillation or severe mitral or aortic valve regurgitation at the time of the echocardiogram. A total of 388 patients met the inclusion criteria. The mean age of the cohort was 67±12 years, with a female (57%) predominance. Prevalence of renal insufficiency (estimated glomerular filtration rate <60 mL/min per 1.73 m(2)) was 34%. The 3-year cumulative probabilities of development of (stage C) HF, development of atrial fibrillation, cardiac hospitalization, and mortality were 11.6%, 14.5%, 17.7%, and 10.1% respectively. In multivariable Cox proportional hazard regression analysis, we determined that age, renal dysfunction, and right ventricular systolic pressure were independently associated with the development of HF.
Conclusions: This population-based study demonstrated that in PDD (stage B) HF, there was a moderate degree of progression to symptomatic (stage C) HF over 3 years, and renal dysfunction was associated with this progression independent of age, sex, hypertension, coronary disease, and ejection fraction.
Figures



References
-
- Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson TB, Flegal K, Ford E, Furie K, Go A, Greenlund K, Haase N, Hailpern S, Ho M, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott M, Meigs J, Mozaffarian D, Nichol G, O’Donnell C, Roger V, Rosamond W, Sacco R, Sorlie P, Stafford R, Steinberger J, Thom T, Wasserthiel-Smoller S, Wong N, Wylie-Rosett J, Hong Y. Heart disease and stroke statistics--2009 update: A report from the american heart association statistics committee and stroke statistics subcommittee. Circulation. 2009;119:e21–181. - PubMed
-
- Senni M, Redfield MM. Heart failure with preserved systolic function. A different natural history? J Am Coll Cardiol. 2001;38:1277–1282. - PubMed
-
- Chen HH, Lainchbury JG, Senni M, Bailey KR, Redfield MM. Diastolic heart failure in the community: Clinical profile, natural history, therapy, and impact of proposed diagnostic criteria. J Card Fail. 2002;8:279–287. - PubMed
-
- Bursi F, Weston SA, Redfield MM, Jacobsen SJ, Pakhomov S, Nkomo VT, Meverden RA, Roger VL. Systolic and diastolic heart failure in the community. JAMA. 2006;296:2209–2216. - PubMed
-
- Redfield MM, Jacobsen SJ, Burnett JC, Jr., Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: Appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
