

Which is the best alternative for displaced femoral neck fractures in the elderly?: A meta-analysis
- PMID: 22278852
- PMCID: PMC3348330
- DOI: 10.1007/s11999-012-2250-6
Which is the best alternative for displaced femoral neck fractures in the elderly?: A meta-analysis
Abstract
Background: Treatment of displaced femoral neck fractures includes internal fixation and arthroplasty. However, whether arthroplasty or internal fixation is the primary treatment for displaced femoral neck fractures in elderly patients remains a subject for debate. The literature contains conflicting evidence regarding rates of mortality, revision surgery, major postoperative complications, and function in elderly patients with displaced femoral neck fractures treated either by internal fixation or arthroplasty (either hemiarthroplasty or THA).
Questions/purpose: We determined mortality, revision surgery rates, major surgical complications (which include infection, nonunion or early redisplacement, avascular necrosis, dislocation, loosening of the prosthesis, acetabular erosion, fracture below or around the implant, and other severe general complications such as deep vein thrombosis and pulmonary embolism), and function in patients treated with either internal fixation or arthroplasty for displaced femoral neck fractures in the elderly.
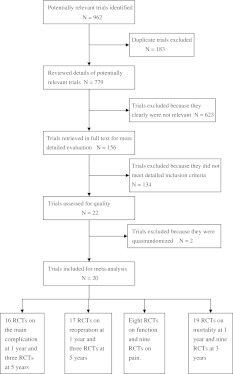
Methods: We searched PubMed, Embase, and the Cochrane Library for randomized controlled trials (RCTs) comparing internal fixation and arthroplasty. We identified 20 RCTs with 4508 patients meeting all the criteria for eligibility. We performed a meta-analysis of the major complications, reoperations, function, pain, and mortality.
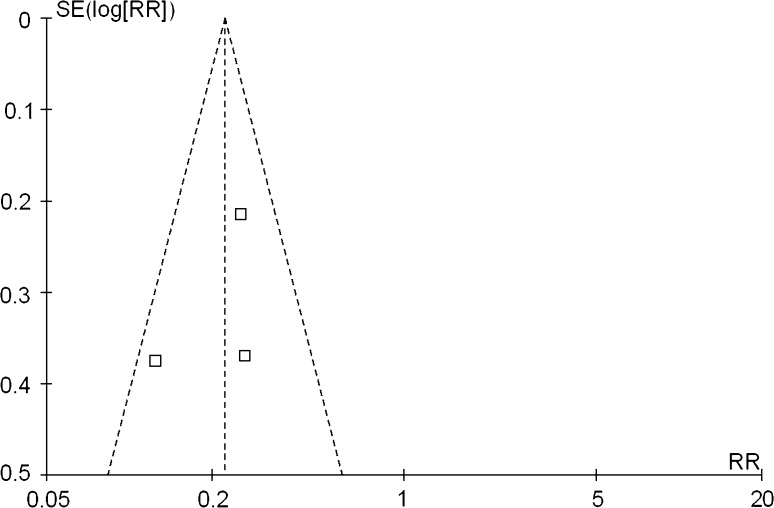
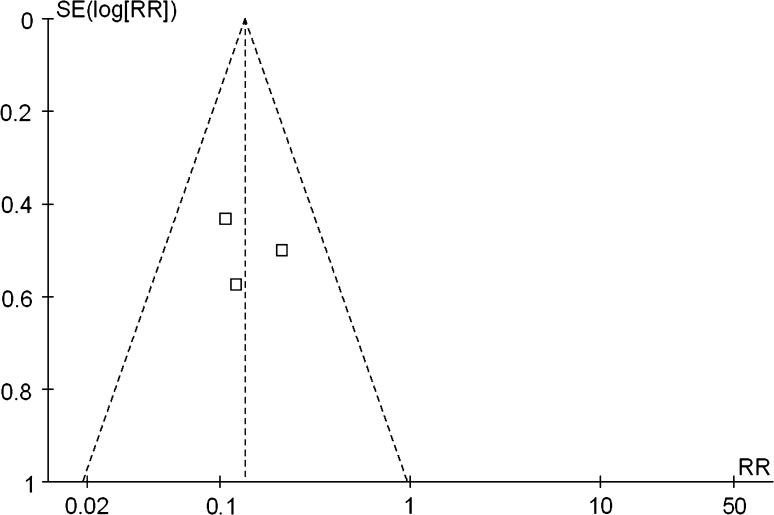
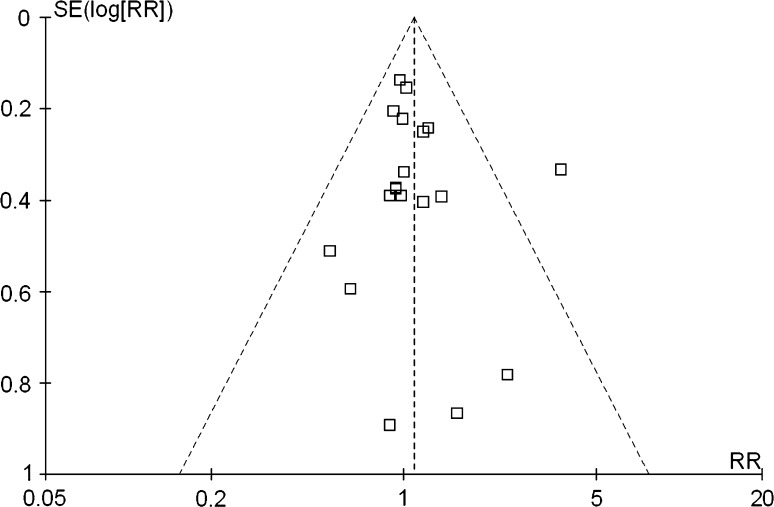
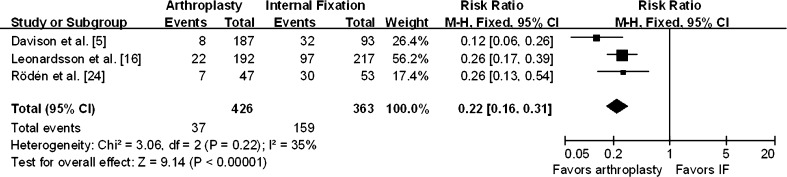
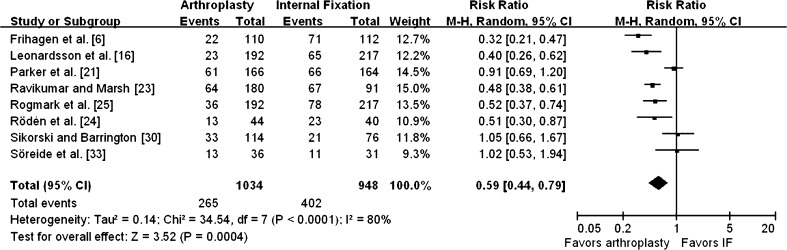
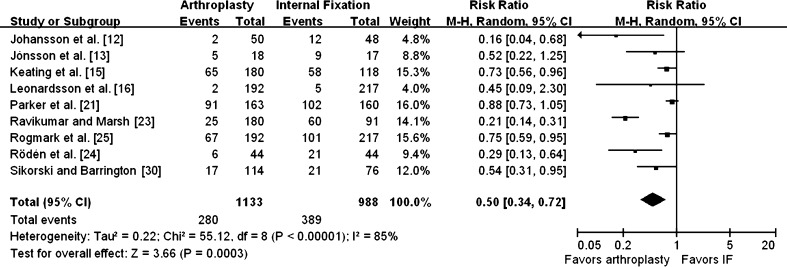
Results: Compared with internal fixation, arthroplasty reduced the risk of the major complications (95% CI, 0.21-0.54 for 1 year; 95% CI, 0.16-0.31 for 5 years) and the incidence of reoperation 1 to 5 years after surgery (95% CI, 0.15-0.34 for 1 year; 95% CI, 0.08-0.24 for 5 years), and provided better pain relief (95% CI, 0.34-0.72). Function was superior (RR = 0.59; 95% CI, 0.44-0.79) for patients treated with arthroplasty than for patients treated by internal fixation. However, mortality 1 to 3 years after surgery was similar (95% CI, 0.96-1.23, p = 0.20 for 1 year; 95% CI, 0.91-1.17, p = 0.63 for 3 years).
Conclusions: Arthroplasty can reduce the risk of major complications and the incidence of reoperation compared with internal fixation, and provide better pain relief and function, but it does not reduce mortality.
Level of evidence: Level II, prognostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Figures





Similar articles
-
Does Arthroplasty Provide Better Outcomes Than Internal Fixation At Mid- and Long-term Followup? A Meta-analysis.Clin Orthop Relat Res. 2015 Aug;473(8):2672-9. doi: 10.1007/s11999-015-4345-3. Epub 2015 May 16. Clin Orthop Relat Res. 2015. PMID: 25981713 Free PMC article. Review.
-
Internal fixation compared with arthroplasty for displaced fractures of the femoral neck. A meta-analysis.J Bone Joint Surg Am. 2003 Sep;85(9):1673-81. doi: 10.2106/00004623-200309000-00004. J Bone Joint Surg Am. 2003. PMID: 12954824
-
Total hip arthroplasty: optimal treatment for displaced femoral neck fractures in elderly patients.Clin Orthop Relat Res. 2004 Dec;(429):43-8. Clin Orthop Relat Res. 2004. PMID: 15577464
-
Primary arthroplasty is better than internal fixation of displaced femoral neck fractures: a meta-analysis of 14 randomized studies with 2,289 patients.Acta Orthop. 2006 Jun;77(3):359-67. doi: 10.1080/17453670610046262. Acta Orthop. 2006. PMID: 16819672 Review.
-
Hemiarthroplasty versus total arthroplasty for displaced femoral neck fractures in the elderly: meta-analysis of randomized clinical trials.Arch Orthop Trauma Surg. 2020 Nov;140(11):1695-1704. doi: 10.1007/s00402-020-03409-3. Epub 2020 Mar 13. Arch Orthop Trauma Surg. 2020. PMID: 32170452
Cited by
-
Does Arthroplasty Provide Better Outcomes Than Internal Fixation At Mid- and Long-term Followup? A Meta-analysis.Clin Orthop Relat Res. 2015 Aug;473(8):2672-9. doi: 10.1007/s11999-015-4345-3. Epub 2015 May 16. Clin Orthop Relat Res. 2015. PMID: 25981713 Free PMC article. Review.
-
Reduced risk of reoperation after treatment of femoral neck fractures with total hip arthroplasty.Acta Orthop. 2017 Oct;88(5):500-504. doi: 10.1080/17453674.2017.1348095. Epub 2017 Jul 10. Acta Orthop. 2017. PMID: 28691547 Free PMC article.
-
Does a hip fracture mean we should we operate on a concomitant proximal humerus fracture?Eur J Orthop Surg Traumatol. 2023 Dec;33(8):3435-3441. doi: 10.1007/s00590-023-03529-7. Epub 2023 May 15. Eur J Orthop Surg Traumatol. 2023. PMID: 37184596
-
Curative efficacy of surgical procedures for older patients with femoral neck fracture: a network meta-analysis and systematic review.J Orthop Surg Res. 2022 Mar 2;17(1):127. doi: 10.1186/s13018-022-02914-y. J Orthop Surg Res. 2022. PMID: 35236384 Free PMC article.
-
Improved outcome after hip fracture surgery in Norway.Acta Orthop. 2017 Oct;88(5):505-511. doi: 10.1080/17453674.2017.1344456. Epub 2017 Jul 6. Acta Orthop. 2017. PMID: 28681677 Free PMC article.
References
-
- Bhandari M, Devereaux PJ, Swiontkowski MF, Tornetta P, 3rd, Obremskey W, Koval KJ, Nork S, Sprague S, Schemitsch EH, Guyatt GH. Internal fixation compared with arthroplasty for displaced fractures of the femoral neck: a meta-analysis. J Bone Joint Surg Am. 2003;85:1673–1681. - PubMed
-
- Bjorgul K, Reikeras O. Hemiarthroplasty in worst cases is better than internal fixation in best cases of displaced femoral neck fractures: a prospective study of 683 patients treated with hemiarthroplasty or internal fixation. Acta Orthop. 2006;77:368–374. doi: 10.1080/17453670610046271. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
