

Surgical outcome of partial Shone complex
- PMID: 22279117
- PMCID: PMC3309834
- DOI: 10.1093/icvts/ivr169
Surgical outcome of partial Shone complex
Abstract
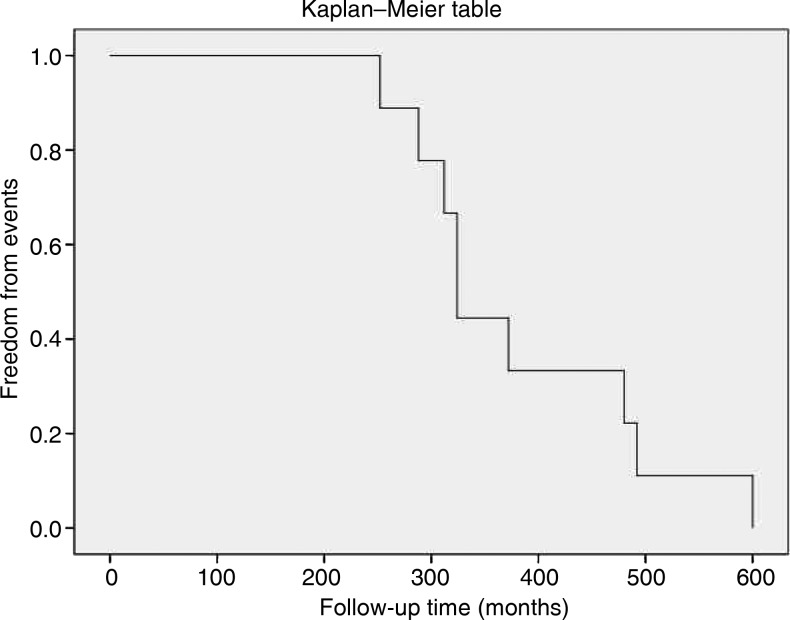
Partial forms of Shone complex are rare. Surgical outcomes of the complete forms have generally been poor, whereas there is a lack of data on long-term follow-up of surgically treated adult partial complex. Between 2001 and 2011, nine patients (age: 38 ± 8 years; six males, 67%) were referred for valvular heart disease. Transthoracic and transoesophageal echocardiography was performed. Data were confirmed by intra-operative findings and reports. Patients were diagnosed as partial Shone complex and presented with mitral stenosis (MS) (45%) or mitral regurgitation (22%) or aortic regurgitation (22%). All but one patient (89%) reported previous surgery: coarctation of the aorta repair (87.5%) and aortic valvulotomy (12.5%). Redo intervention included: mitral valve replacement (25%), mitral repair (25%), aortic valve replacement (37.5%) and subvalvular aortic ridge resection (25%). One patient refused surgery. Patients surgically treated before the age of 5 (87.5%) showed favourable outcome (survival rate: 100%) and a 23.6 (± 4.6)-year follow-up free from events. The patient who underwent first intervention at the age of 50 and the patient with MS who refused surgery showed a 45 (± 7)-year follow-up free from major morbidity. Patients with partial Shone complex, properly diagnosed and treated, show favourable surgical outcome free from major clinical events.
Figures



References
-
- Shone JD, Sellers RD, Anderson RC, Adams P, Jr, Lillehei CW, Edwards JE. The developmental complex of ‘parachute mitral valve,’ supravalvular ring of left atrium, subaortic stenosis, and coarctation of aorta. Am J Cardiol. 1963;11:714–25. doi:10.1016/0002-9149(63)90098-5. - DOI - PubMed
-
- Purvis JA, Smyth S, Barr SH. Multi-modality imaging of an adult parachute mitral valve. J Am Soc Echocardiogr. 2010;24:351. - PubMed
-
- Becker AE, Becker MJ, Edwards JE. Anomalies associated with coarctation of aorta; particular reference to infancy. Circulation. 1970;41:1067–75. - PubMed
-
- Davachi F, Moller JH, Edwards JE. Diseases of the mitral valve in infancy. An anatomic analysis of 55 cases. Circulation. 1971;43:565–79. - PubMed
-
- Hakim FA, Kendall CB, Alharthi M, Mancina JC, Tajik JA, Mookadam F. Parachute mitral valve in adults-a systematic overview. Echocardiography. 2010;27:581–86. doi:10.1111/j.1540-8175.2009.01143.x. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
