Dysfunctional voiding: A review of the terminology, presentation, evaluation and management in children and adults
- PMID: 22279306
- PMCID: PMC3263208
- DOI: 10.4103/0970-1591.91429
Dysfunctional voiding: A review of the terminology, presentation, evaluation and management in children and adults
Abstract
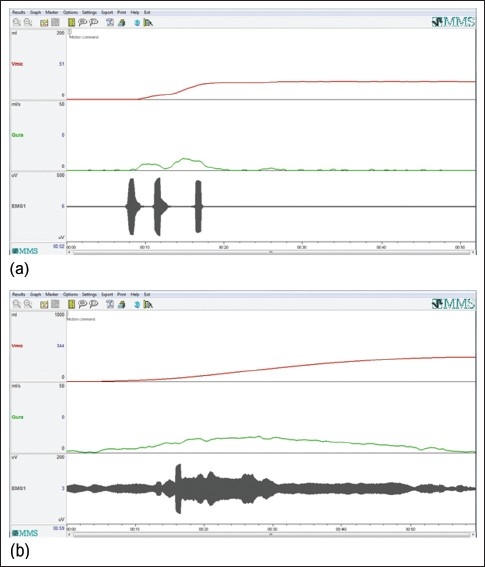
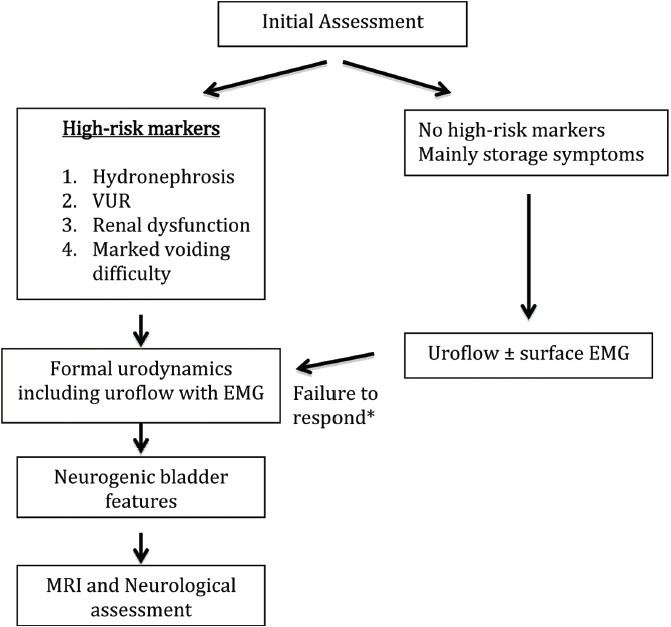
Dysfunctional voiding (DV) is a voiding disorder characterized by dyssynergic striated sphincteric activity in the absence of a proven neurological etiology. It can present at any age with a spectrum of storage and voiding symptoms that may resemble florid neurogenic bladder. There is a striking lack of clarity regarding what this entity represents, the diagnostic methodology and treatment. The limitations of existing guideline documents are analyzed. Specifically, use of the term "habitual", the assumption that bladder changes are secondary to the outlet, the emphasis on "staccato" voiding and the implication of striated urethral sphincter are discussed. Literature shows that DV may also present with continuous slow flow or normal flow. Dyssynergia may be at the level of the striated urethral sphincter, the pelvic floor or both, better termed "striated urethral sphincter-pelvic floor complex" (SUS-PFC).A diagnostic algorithm is provided so that patients are evaluated on merit rather than on the basis of different philosophies of individual centers. High-risk markers such as hydronephrosis, vesicoureteral reflux, renal failure or marked voiding difficulty should prompt a formal urodynamics evaluation and imaging for neurological etiology. Patients with predominantly storage symptoms with incidental staccato voiding can be managed initially, on the basis of non-invasive evaluation. Conservative urotherapy including biofeedback is appropriate initial management for patients without high risk factors. Treatment and evaluation should be escalated based on response. Patients with severe DV will need treatment similar to neurogenic bladder including clean intermittent catheterization and measures to control storage pressures.
Keywords: Dysfunctional voiding; International Children's Continence Society; International Continence Society; guidelines; staccato voiding; terminology; urodynamics; uroflow.
Conflict of interest statement
Figures
Similar articles
-
Analysis of uroflow patterns in children with dysfunctional voiding.J Pediatr Urol. 2014 Apr;10(2):250-4. doi: 10.1016/j.jpurol.2013.10.010. Epub 2013 Nov 7. J Pediatr Urol. 2014. PMID: 24290223
-
Diaphragmatic breathing exercises and pelvic floor retraining in children with dysfunctional voiding.Eur J Phys Rehabil Med. 2012 Sep;48(3):413-21. Epub 2012 Jun 5. Eur J Phys Rehabil Med. 2012. PMID: 22669134 Clinical Trial.
-
Exploring dysfunctional voiding in girls: a comprehensive literature review of assessment and management strategies.BMC Urol. 2025 Apr 12;25(1):87. doi: 10.1186/s12894-025-01772-0. BMC Urol. 2025. PMID: 40221717 Free PMC article. Review.
-
Can staccato and interrupted/fractionated uroflow patterns alone correctly identify the underlying lower urinary tract condition?J Urol. 2012 Jun;187(6):2188-93. doi: 10.1016/j.juro.2012.01.126. Epub 2012 Apr 12. J Urol. 2012. PMID: 22503030
-
Dysfunctional Voiding in Pediatrics: A Review of Pathophysiology and Current Treatment Modalities.Curr Pediatr Rev. 2016;12(4):292-300. doi: 10.2174/1573396312666160816163020. Curr Pediatr Rev. 2016. PMID: 27539311 Review.
Cited by
-
Prevalence of Lower Urinary Tract Symptoms in Children with Attention-Deficit/Hyperactivity Disorder: Comparison of Hospital and Population-Based Cohorts of 13,000 Patients.J Clin Med. 2022 Oct 28;11(21):6393. doi: 10.3390/jcm11216393. J Clin Med. 2022. PMID: 36362621 Free PMC article.
-
Is urotherapy alone as effective as a combination of urotherapy and biofeedback in children with dysfunctional voiding?Int Braz J Urol. 2018 Sep-Oct;44(5):987-995. doi: 10.1590/S1677-5538.IBJU.2018.0194. Int Braz J Urol. 2018. PMID: 30130020 Free PMC article.
-
Voiding Dysfunction Due to Urethral Sphincter Dysfunction Might Be an Early Neurological Presentation of Central Nervous System Disorders in Aged Patients.J Pers Med. 2023 Apr 20;13(4):693. doi: 10.3390/jpm13040693. J Pers Med. 2023. PMID: 37109078 Free PMC article.
-
Botulinum Toxin A and Lower Urinary Tract Dysfunction: Pathophysiology and Mechanisms of Action.Toxins (Basel). 2016 Apr 21;8(4):120. doi: 10.3390/toxins8040120. Toxins (Basel). 2016. PMID: 27110822 Free PMC article. Review.
-
Correlation Between Apical, Anterior, and Posterior Vaginal Wall Prolapse With Voiding Dysfunction: A Single Center Retrospective Cohort Study.J Family Reprod Health. 2024 Jun;18(2):115-121. doi: 10.18502/jfrh.v18i2.15935. J Family Reprod Health. 2024. PMID: 39011415 Free PMC article.
References
-
- Fan YH, Lin AT, Wu HM, Hong CJ, Chen KK. Psychological profile of female patients with dysfunctional voiding. Urology. 2008;71:625–9. - PubMed
-
- Adams J, Mehls O, Wiesel M. Pediatric renal transplantation and the dysfunctional bladder. Transpl Int. 2004;17:596–602. - PubMed
-
- Glassberg KI, Combs AJ, Horowitz M. Nonneurogenic voiding disorders in children and adolescents: Clinical and videourodynamic findings in 4 specific conditions. J Urol. 2010;184:2123–7. - PubMed
-
- Beer E. Chronic retention of urine in children. JAMA. 1915;65:1709.
-
- Allen TD. Non-neurogenic neurogenic bladder. J Urol. 1977;177:232–8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous