

In papillary thyroid cancer, preoperative central neck ultrasound detects only macroscopic surgical disease, but negative findings predict excellent long-term regional control and survival
- PMID: 22280230
- PMCID: PMC3968956
- DOI: 10.1089/thy.2011.0121
In papillary thyroid cancer, preoperative central neck ultrasound detects only macroscopic surgical disease, but negative findings predict excellent long-term regional control and survival
Abstract
Background: Ultrasound (US) of the central neck compartment (CNC) is considered of limited sensitivity for nodal spread in papillary thyroid cancer (PTC); elective neck dissection is commonly advocated even in the absence of sonographic abnormalities. We hypothesized that US is an accurate predictor for long-term disease-free survival, regardless of the use of elective central neck dissection in patients with PTC.
Methods: A retrospective chart review of 331 consecutive PTC patients treated with total thyroidectomy at M.D. Anderson Cancer Center between 1996 and 2003 was performed. Information retrieved included preoperative sonographic status of the CNC, surgical treatment of the neck, demographics, cancer staging, histopathological variables and use of adjuvant treatment. The endpoints for the study were nodal recurrence and survival.
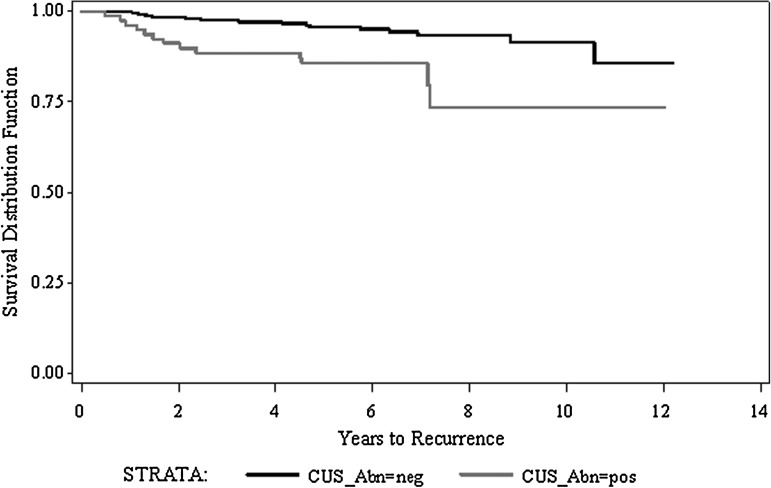
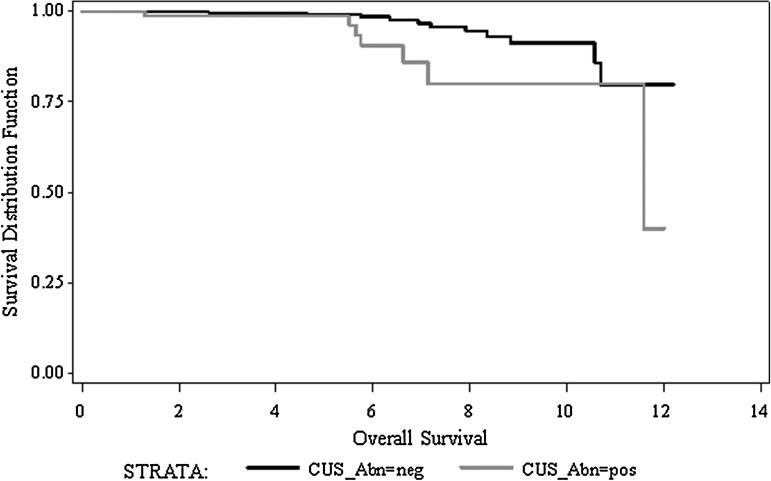
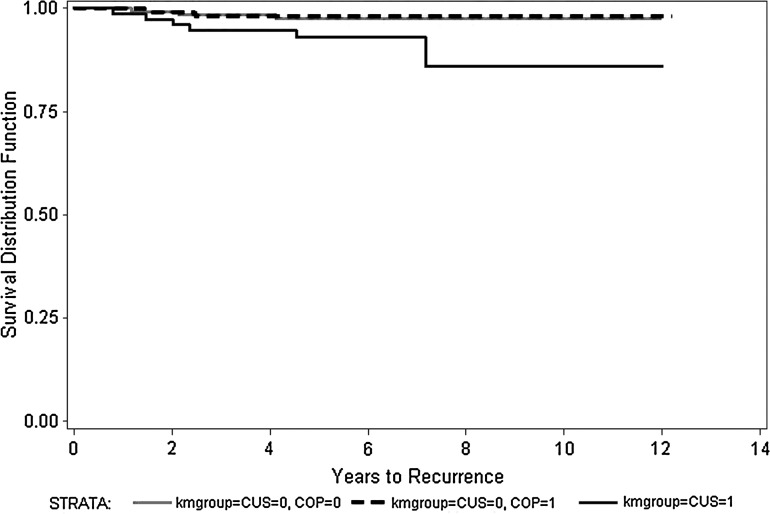
Results: There were 112 males and 219 females with a median age of 44 years (range 11-87). The median follow-up time for the series was 71.5 months (range 12.7-148.7). There were 151 (45.6%) patients with a T1, 58 (17.5%) with a T2, 70 (21.1%) with a T3, and 52 (15.7%) with a T4. Preoperative sonographic abnormalities were present in the CNC in 79 (23.9%) patients. During the surveillance period, 11 (3.2%) patients recurred in the central neck, with an average time for recurrence of 22.8 months. Advanced T stage (T3/T4) and abnormal US were independent prognostic factors for recurrence in the central neck (p=0.013 and p=0.005 respectively). There were 119 (35%) patients with a sonographically negative central compartment who underwent elective central neck dissection; 85 of them (71.4%) were found to be histopathologically N(+) while 34 (28.6%) were pN0. There were no differences in overall survival (p=0.32), disease specific survival (DSS; p=0.49), and recurrence-free survival (p=0.32) between these two groups. Preoperative US of the CNC was an age-independent predictor for overall survival (p<0.001), DSS (p=0.0097), and disease-free survival (p=0.0005) on bivariate Cox regression.
Conclusions: US of the central compartment is an age-independent predictor for survival and CNC recurrence-free survival in PTC. Prophylactic neck dissection of the central compartment does not improve long-term disease control, regardless of the histopathological status of the lymph nodes retrieved. Our findings emphasize the ability of US to clinically detect relevant nodal disease and support conservative management of the CNC in the absence of abnormal findings.
Figures
Comment in
-
Prophylactic central neck dissection in differentiated thyroid cancer: a procedure in search of an indication.Thyroid. 2012 Apr;22(4):341-3. doi: 10.1089/thy.2012.2204.ed. Thyroid. 2012. PMID: 22458971 No abstract available.
References
-
- Heller KS. Do all cancers need to be treated? The role of thyroglobulin in the management of thyroid cancer: the 2006 Hayes Martin lecture. Arch Otolaryngol Head Neck Surg. 2007;133:639–643. - PubMed
-
- Cooper DS. Doherty GM. Haugen BR. Kloos RT. Lee SL. Mandel SJ. Mazzaferri EL. McIver B. Sherman SI. Tuttle RM. Management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2006;16:109–142. - PubMed
-
- Mazzaferri EL. Management of a solitary thyroid nodule. N Engl J Med. 1993;328:553–559. - PubMed
-
- Lundgren CI. Hall P. Dickman PW. Zedenius J. Clinically significant prognostic factors for differentiated thyroid carcinoma: a population-based, nested case-control study. Cancer. 2006;106:524–531. - PubMed
-
- Kupferman ME. Patterson DM. Mandel SJ. LiVolsi V. Weber RS. Safety of modified radical neck dissection for differentiated thyroid carcinoma. Laryngoscope. 2004;114:403–406. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
