

Surgical treatment of drug-resistant tuberculosis
- PMID: 22281142
- PMCID: PMC3741680
- DOI: 10.1016/S1473-3099(11)70244-4
Surgical treatment of drug-resistant tuberculosis
Abstract
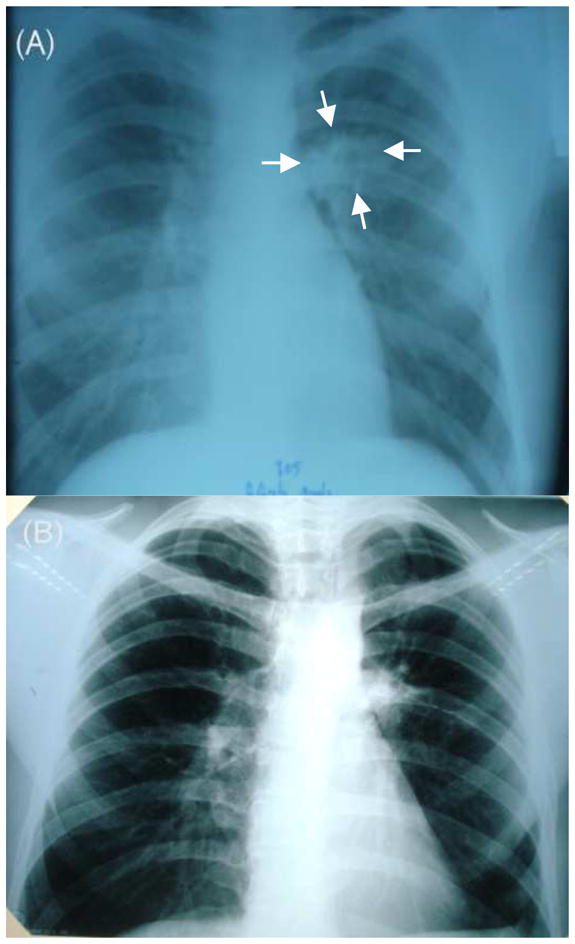
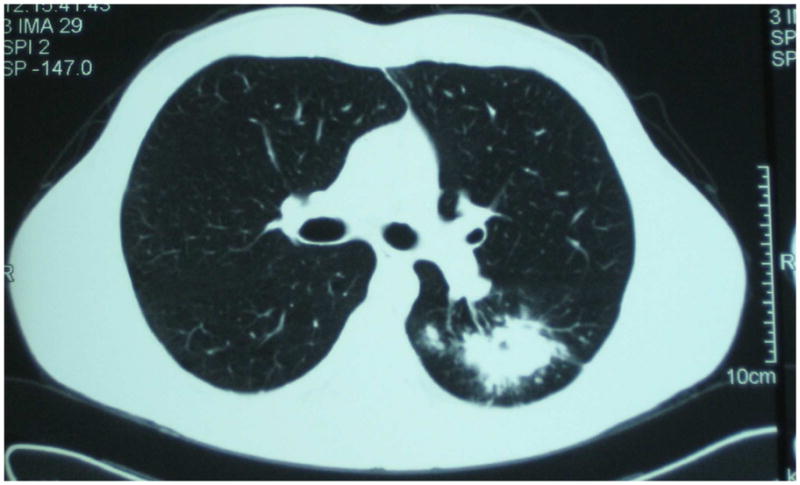
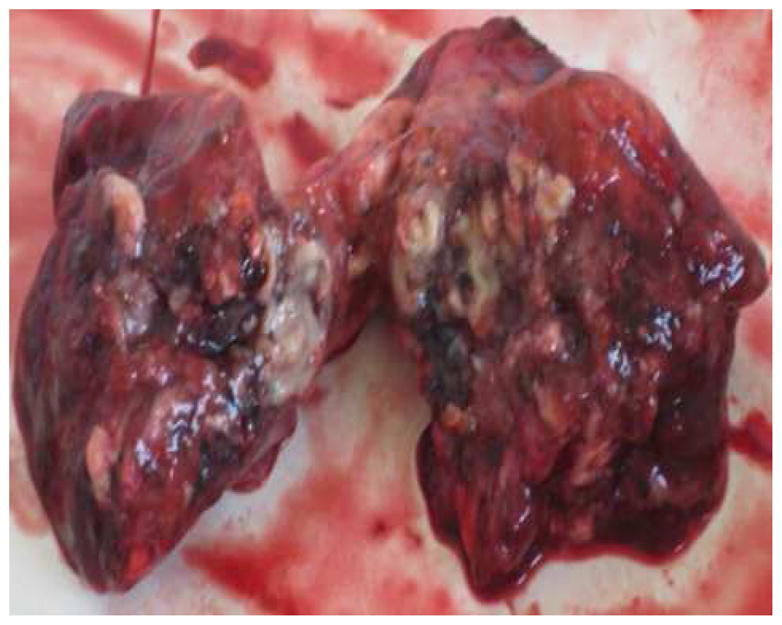
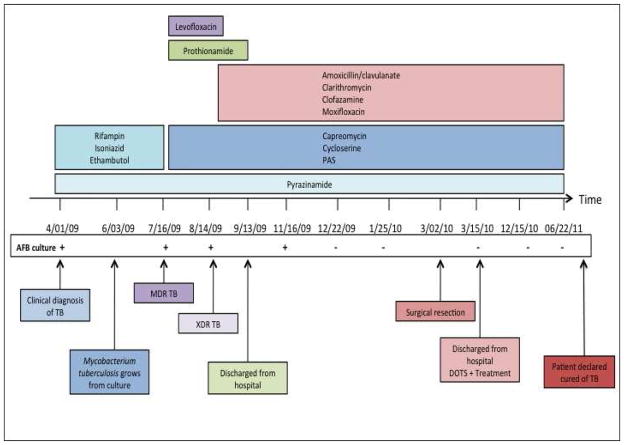
The global emergence and spread of multidrug-resistant (MDR) and extensively drug-resistant (XDR) tuberculosis has led to the re-examination of surgery as a possible adjunctive treatment. We present the case of a 26-year-old HIV-seronegative patient with XDR pulmonary tuberculosis refractory to medical therapy. Surgical resection of the patient's solitary cavitary lesion was done as adjunctive treatment, and a successful outcome with a combination of surgery and drug therapy was achieved. We review the history of surgical therapy for tuberculosis and reports of its role in treatment of MDR and XDR tuberculosis. 26 case series and cohort studies were included, and together showed that surgical resection is beneficial in the treatment of drug-resistant tuberculosis. However, the results might not be applicable in all settings because investigations were observational and typically included patients with less severe disease, and all surgeries were done at specialised thoracic-surgery centres. Well designed studies are needed to establish the efficacy of surgery in treatment of drug-resistant tuberculosis.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
We declare that we have no conflicts of interest.
Figures
References
-
- Koch R. Classics in infectious diseases. The etiology of tuberculosis: Robert Koch. Berlin, Germany 1882. Rev Infect Dis. 1982;4:1270–4. - PubMed
-
- Sihoe AD, Shiraishi Y, Yew WW. The current role of thoracic surgery in tuberculosis management. Respirology. 2009;14:954–68. - PubMed
-
- Perelman MI, Strelzov VP. Surgery for pulmonary tuberculosis. World J Surg. 1997;21:457–67. - PubMed
-
- Tuffier T. De la resection du sommet du poumon. Semin Med. 1891;11:202.
-
- WHO. WHO/HTM/TB/20103. Geneva: World Health Organization; 2010. Multidrug and extensively drug-resistant TB (M/XDR-TB): 2010 global report on surveillance and response.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
