

The posterior location of the dilator muscle induces anterior iris bowing during dilation, even in the absence of pupillary block
- PMID: 22281822
- PMCID: PMC3339903
- DOI: 10.1167/iovs.11-8408
The posterior location of the dilator muscle induces anterior iris bowing during dilation, even in the absence of pupillary block
Abstract
Purpose: To examine the effect of the posterior location of the dilator on iris anterior curvature during dilation.
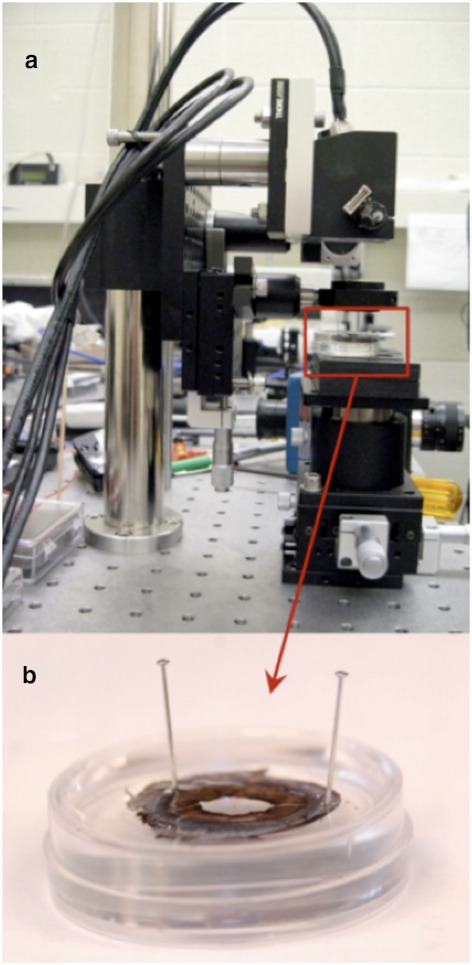
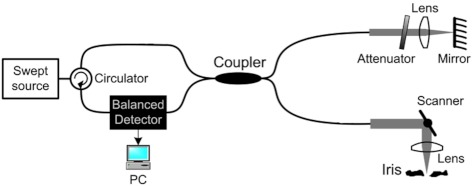
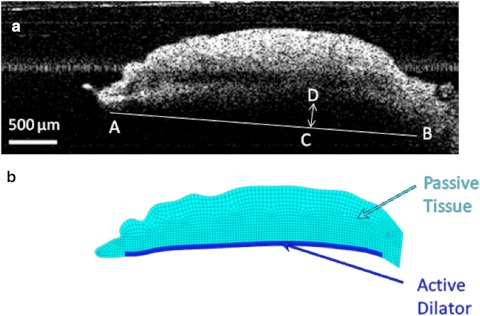
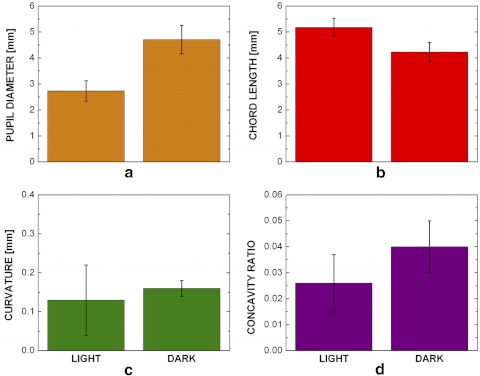
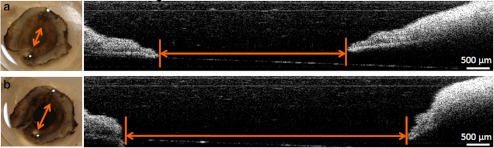
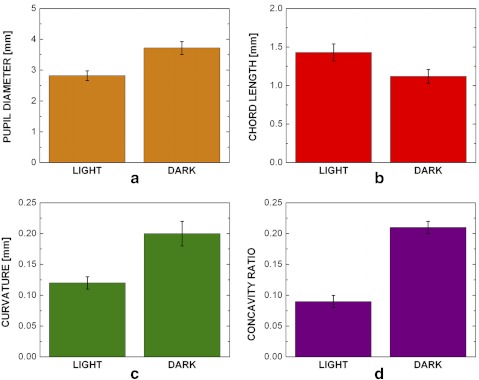
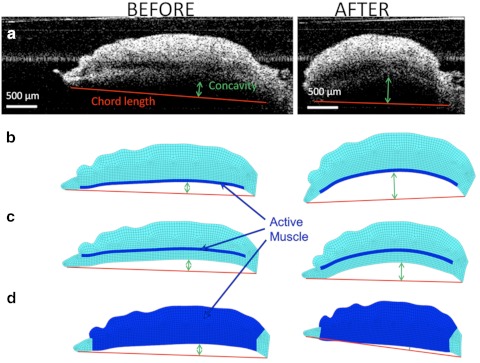
Methods: An in vivo human study, an ex vivo porcine experiment, and an in silico computational model were performed in parallel. Iris anterior curvature was measured in vivo before and after dilation by time-domain slit lamp optical coherence tomography (SL-OCT). All patients (n = 7) had undergone laser peripheral iridotomy to eliminate any pupillary block due to primary angle-closure glaucoma. In the ex vivo experiments, isolated porcine irides (n = 30) were secured at the periphery and immersed in an oxygenated Krebs-Ringer buffer. Dilation was induced pharmaceutically by the addition of 2.5% phenylephrine and 1% tropicamide. An in-house optical coherence tomography (OCT) system was used to obtain iris images before and after dilation. A finite element model was also developed based on typical geometry of the iris from the initial OCT image. The iris was modeled as a neo-Hookean solid, and the active muscle component was applied only to the region specified as the dilator.
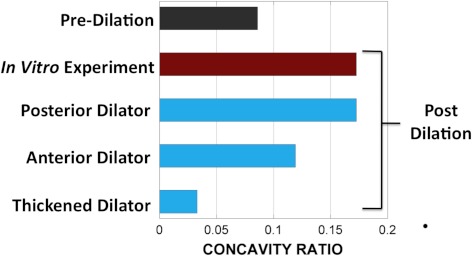
Results: An increase in curvature and a decrease in chord length after dilation were observed in both experiments. In both the in vivo and ex vivo experiments, the curvature-to-chord length ratio increased significantly during dilation. Computer simulations agreed well with the experimental results only when the proper anatomic position of dilator was used.
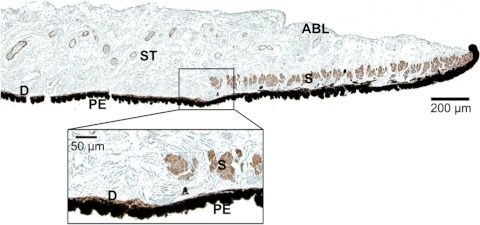
Conclusions: The posterior location of the dilator contributes to the anterior iris bowing via a nonpupillary block dependent mechanism.
Figures
References
-
- Mandell MA, Pavlin CJ, Weisbrod DJ, Simpson ER. Anterior chamber depth in plateau iris syndrome and pupillary block as measured by ultrasound biomicroscopy. Am J Ophthalmol. 2003;136:900–903 - PubMed
-
- Nonaka A, Iwawaki T, Kikuchi M, Fujihara M, Nishida A, Kurimoto Y. Quantitative evaluation of iris convexity in primary angle closure. Am J Ophthalmol. 2007;143:695–697 - PubMed
-
- Ritch LR. Angle-closure glaucoma: mechanisms and epidemiology. The Glaucomas; St. Louis: Mosby; 1996:chap 37
-
- Woo EK, Pavlin CJ, Slomovic A, Taback N, Buys YM. Ultrasound biomicroscopic quantitative analysis of light-dark changes associated with pupillary block. Am J Ophthalmol. 1999;127:43–47 - PubMed
-
- Huang EC, Barocas VH. Active iris mechanics and pupillary block: steady-state analysis and comparison with anatomical risk factors. Ann Biomed Eng. 2004;32:1276–1285 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
