

The epidemiology of intensive care unit readmissions in the United States
- PMID: 22281829
- PMCID: PMC3359937
- DOI: 10.1164/rccm.201109-1720OC
The epidemiology of intensive care unit readmissions in the United States
Abstract
Rationale: The incidence of intensive care unit (ICU) readmissions across the United States is unknown.
Objectives: To determine incidence of ICU readmissions in United States hospitals, and describe the distribution of time between ICU discharges and readmissions.
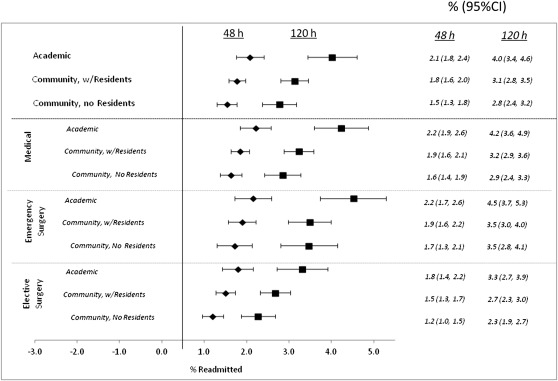
Methods: This retrospective cohort study used 196,202 patients in 156 medical and surgical ICUs in 106 community and academic hospitals participating in Project IMPACT from April 1, 2001, to December 31, 2007. We used mixed-effects logistic regression, adjusting for patient and hospital characteristics, to describe how ICU readmission rates differed across patient types, ICU models, and hospital types.
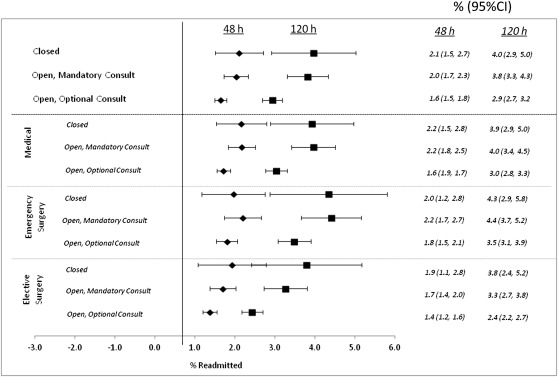
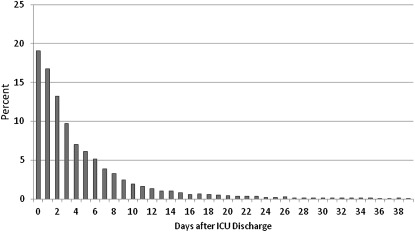
Measurements and main results: Measurements consisted of 48- and 120-hour ICU readmission rates and time to readmission. A total of 3,905 patients (2%) were readmitted to the ICU within 48 hours, and 7,171 (3.7%) within 120 hours. In adjusted analysis, there was no difference in ICU readmissions across patient types or ICU models. Among medical patients, those in academic hospitals had higher odds of 48- and 120-hour readmission than patients in community hospitals without residents (1.51 [95% confidence interval, 1.12-2.02] and 1.63 [95% confidence interval, 1.24-2.16]). Median time to ICU readmission was 3.07 days (interquartile range, 1.27-6.58). Closed ICUs had the longest times to readmission (3.55 d [interquartile range, 1.42-7.50]).
Conclusions: Approximately 2% and 4% of ICU patients discharged to the ward are readmitted within 48 and 120 hours, within a median time of 3 days. Medical patients in academic hospitals are more likely to be readmitted than patients in community hospitals without residents. ICU readmission rates could be useful for policy makers and investigations into their causes and consequences.
Figures
Comment in
-
"She's out of the ICU now." "That's a relief, isn't it?": The growing problem of ICU recidivism.Am J Respir Crit Care Med. 2012 May 1;185(9):906-8. doi: 10.1164/rccm.201201-0152ED. Am J Respir Crit Care Med. 2012. PMID: 22550206 No abstract available.
References
-
- de Vos M, Graafmans W, Keesman E, Westert G, van der Voort PH. Quality measurement at intensive care units: which indicators should we use? J Crit Care 2007;22:267–274 - PubMed
-
- Cooper GS, Sirio CA, Rotondi AJ, Shepardson LB, Rosenthal GE. Are readmissions to the intensive care unit a useful measure of hospital performance? Med Care 1999;37:399–408 - PubMed
-
- Woodhouse D, Berg M, van der Putten J, Houtepen J. Will benchmarking ICUs improve outcome? Curr Opin Crit Care 2009;15:450–455 - PubMed
-
- McMillan TR, Hyzy RC. Bringing quality improvement into the intensive care unit. Crit Care Med 2007;35:S59–S65 - PubMed
-
- Afessa B, Keegan MT, Hubmayr RD, Naessens JM, Gajic O, Long KH, Peters SG. Evaluating the performance of an institution using an intensive care unit benchmark. Mayo Clin Proc 2005;80:174–180 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
