

A phase IIa trial of the new tuberculosis vaccine, MVA85A, in HIV- and/or Mycobacterium tuberculosis-infected adults
- PMID: 22281831
- PMCID: PMC3326425
- DOI: 10.1164/rccm.201108-1548OC
A phase IIa trial of the new tuberculosis vaccine, MVA85A, in HIV- and/or Mycobacterium tuberculosis-infected adults
Abstract
Rationale: Novel tuberculosis (TB) vaccines should be safe and effective in populations infected with Mycobacterium tuberculosis (M.tb) and/or HIV for effective TB control.
Objective: To determine the safety and immunogenicity of MVA85A, a novel TB vaccine, among M.tb- and/or HIV-infected persons in a setting where TB and HIV are endemic.
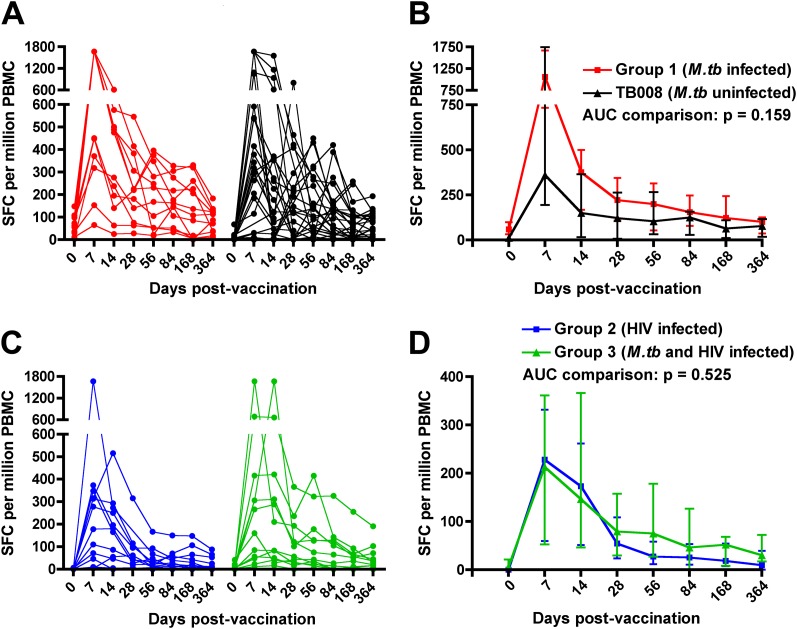
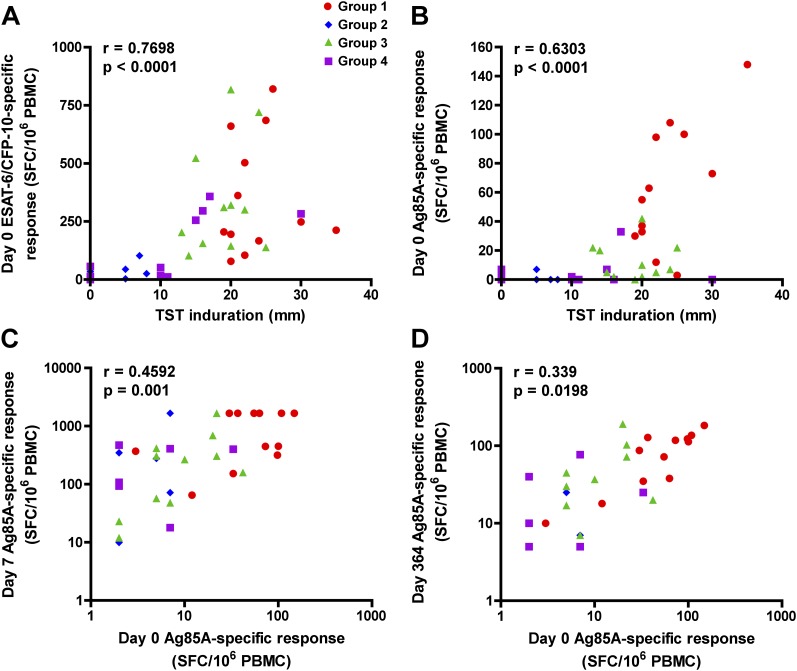
Methods: An open-label, phase IIa trial was conducted in 48 adults with M.tb and/or HIV infection. Safety and immunogenicity were analyzed up to 52 weeks after intradermal vaccination with 5 × 10(7) plaque-forming units of MVA85A. Specific T-cell responses were characterized by IFN-γ enzyme-linked immunospot and whole blood intracellular cytokine staining assays.
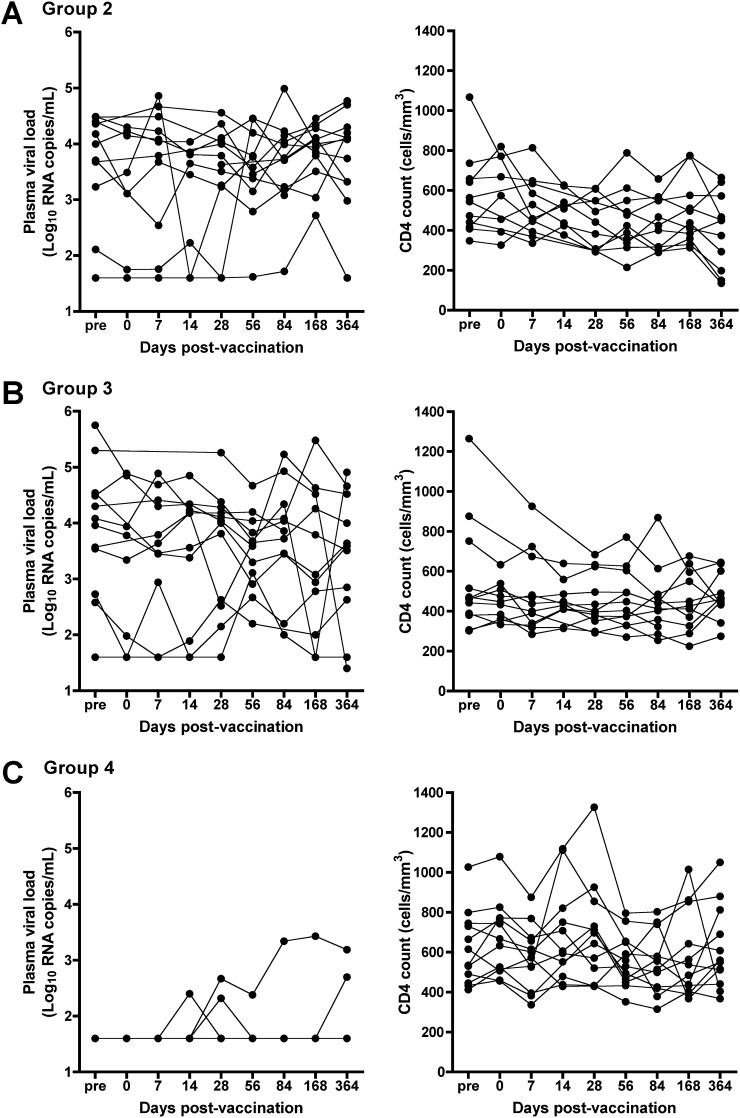
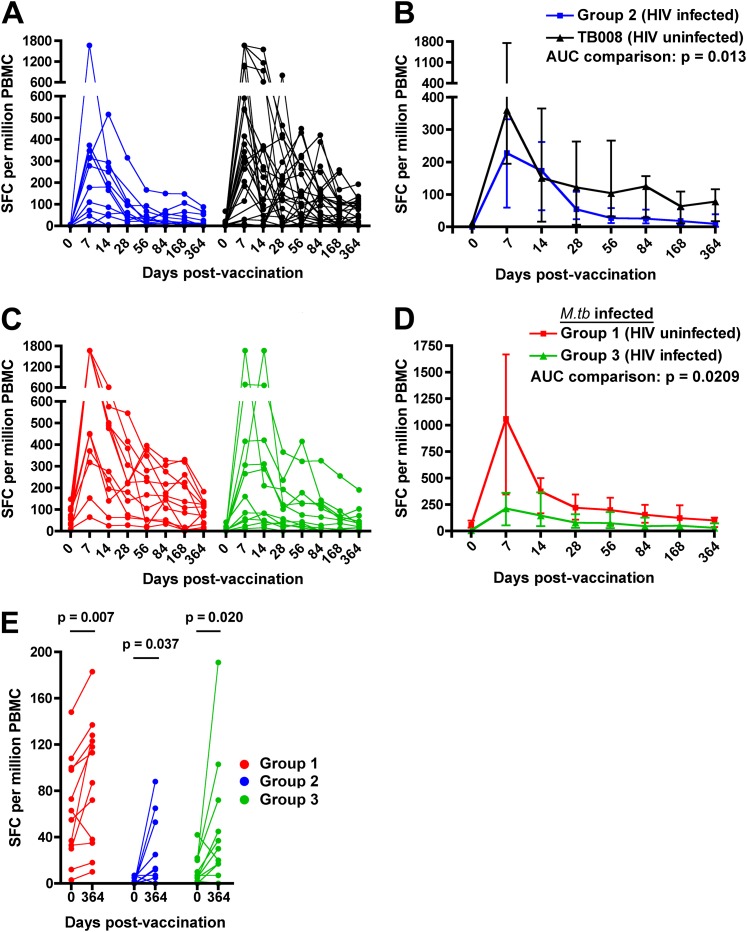
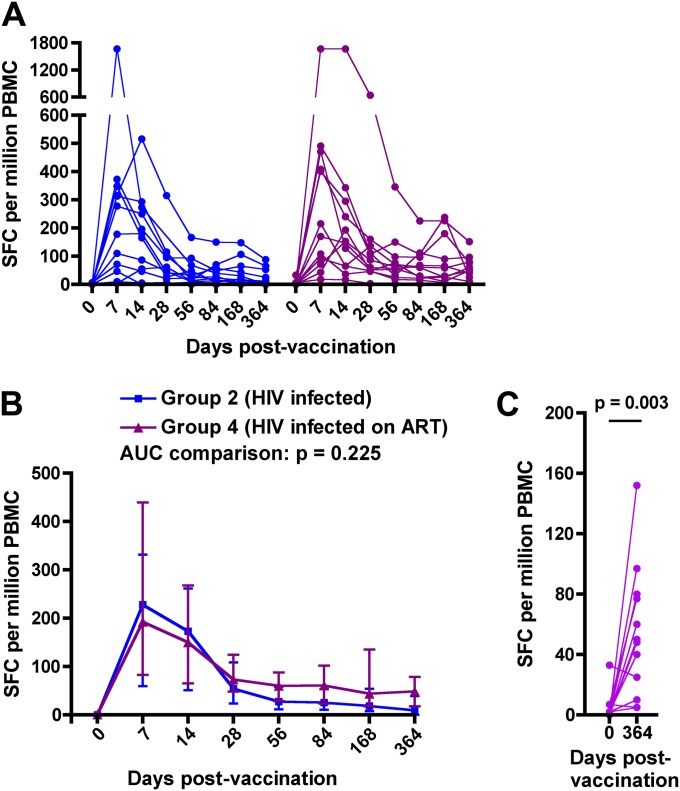
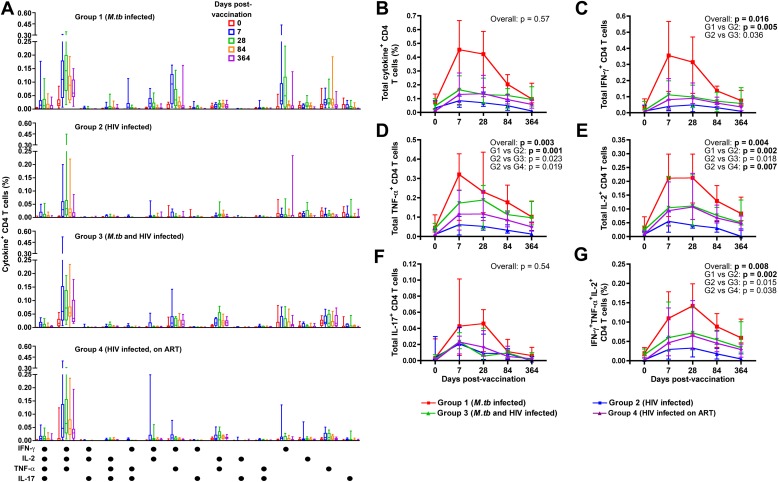
Measurements and main results: MVA85A was well tolerated and no vaccine-related serious adverse events were recorded. MVA85A induced robust and durable response of mostly polyfunctional CD4(+) T cells, coexpressing IFN-γ, tumor necrosis factor-α, and IL-2. Magnitudes of pre- and postvaccination T-cell responses were lower in HIV-infected, compared with HIV-uninfected, vaccinees. No significant effect of antiretroviral therapy on immunogenicity of MVA85A was observed.
Conclusions: MVA85A was safe and immunogenic in persons with HIV and/or M.tb infection. These results support further evaluation of safety and efficacy of this vaccine for prevention of TB in these target populations.
Trial registration: ClinicalTrials.gov NCT00480558.
Figures
References
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, Dye C. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med 2003;163:1009–1021 - PubMed
-
- Rodrigues LC, Diwan VK, Wheeler JG. Protective effect of BCG against tuberculous meningitis and miliary tuberculosis: a meta-analysis. Int J Epidemiol 1993;22:1154–1158 - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
