

Oncogene status predicts patterns of metastatic spread in treatment-naive nonsmall cell lung cancer
- PMID: 22282022
- PMCID: PMC3370097
- DOI: 10.1002/cncr.27409
Oncogene status predicts patterns of metastatic spread in treatment-naive nonsmall cell lung cancer
Abstract
Background: The discovery of distinct subsets of nonsmall cell lung cancer (NSCLC) characterized by activation of driver oncogenes has greatly affected personalized therapy. It is hypothesized that the dominant oncogene in NSCLC would be associated with distinct patterns of metastatic spread in NSCLC at the time of diagnosis.
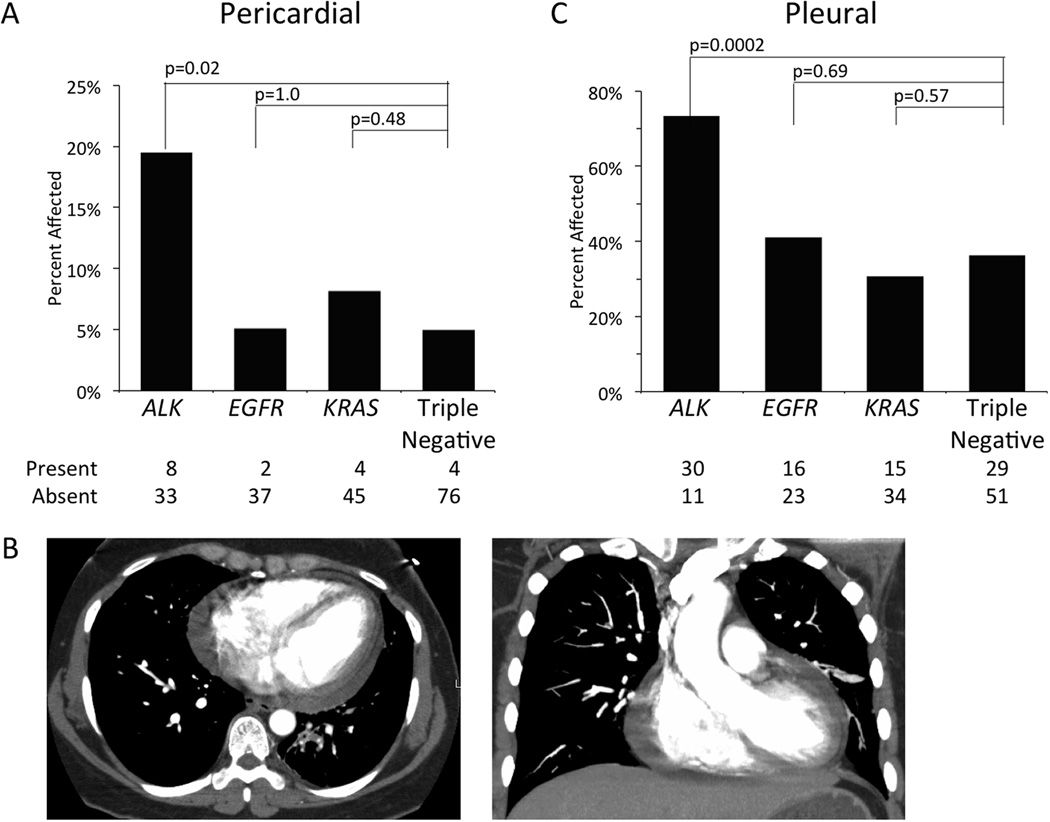
Methods: A total of 209 consecutive patients with stage IV nonsquamous NSCLC with an EGFR (epidermal growth factor receptor) mutation (N = 39), KRAS (v-Ki-ras2 Kirsten rat sarcoma viral oncogene homolog) mutation (N = 49), ALK (anaplastic lymphoma receptor tyrosine kinase) gene rearrangement (N = 41), or wild-type for all 3 (triple negative, N = 80) were included. The percentage of patients with metastatic disease at a given site was compared between each molecular cohort (EGFR, KRAS, or ALK) and the triple negative cohort.
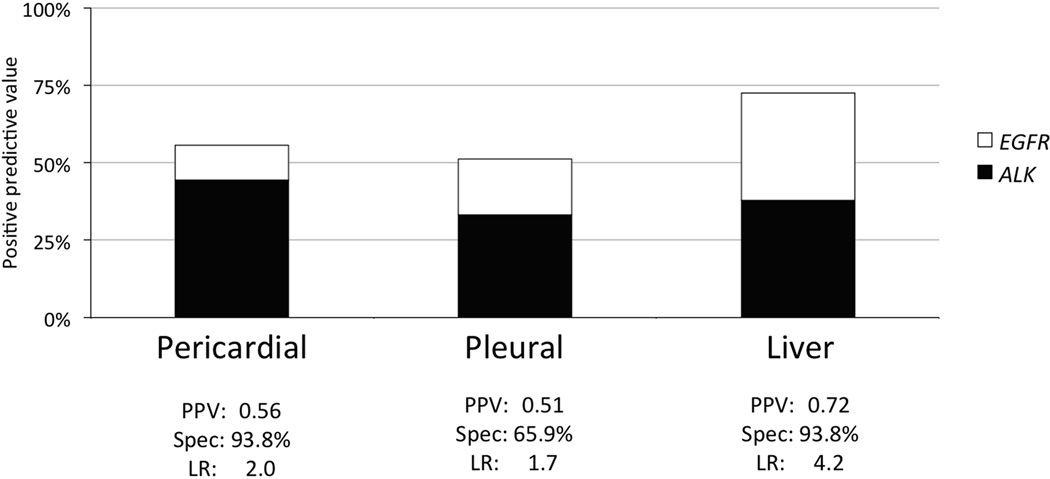
Results: ALK gene rearrangement was significantly associated with pericardial disease (odds ratio [OR] = 4.61; 95% confidence interval [CI] = 1.30, 16.37; P = .02) and pleural disease (OR = 4.80; 95% CI = 2.10, 10.97; P < .001). Patients with ALK gene rearrangements (OR = 5.50; 95% CI = 1.76, 17.18; P = .003) and patients with EGFR mutations (OR = 5.17; 95% CI = 1.63, 16.43; P = .006) were predisposed to liver metastasis compared to the triple negative cohort. No molecular cohort had a predisposition to pulmonary nodules, or adrenal, bone, or brain metastasis compared to the triple negative cohort. The mean number of metastatic disease sites in patients within the ALK rearranged cohort was significantly greater than that of the triple negative cohort (mean = 3.6 sites vs 2.5 sites, P < .0001).
Conclusions: The results support the hypothesis that the dominant molecular oncogenes in NSCLC are associated with different biological behaviors manifesting as distinct patterns of metastatic spread at the time of diagnosis.
Copyright © 2012 American Cancer Society.
Figures




Comment in
-
Lung cancer with translocation in the anaplastic lymphoma kinase gene: a disease within a disease.Cancer. 2012 Sep 15;118(18):4370-1. doi: 10.1002/cncr.27402. Epub 2012 Jan 26. Cancer. 2012. PMID: 22281941 No abstract available.
References
-
- Scagliotti GV, Parikh P, von Pawel J, et al. Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2008;26(21):3543–3551. - PubMed
-
- Sandler A, Gray R, Perry MC, et al. Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancer. The New England journal of medicine. 2006;355(24):2542–2550. - PubMed
-
- Douillard JY, Shepherd FA, Hirsh V, et al. Molecular predictors of outcome with gefitinib and docetaxel in previously treated non-small-cell lung cancer: data from the randomized phase III INTEREST trial. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 2010;28(5):744–752. - PubMed
-
- Lynch TJ, Bell DW, Sordella R, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. The New England journal of medicine. 2004;350(21):2129–2139. - PubMed
-
- Mok TS, Wu YL, Thongprasert S, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. The New England journal of medicine. 2009;361(10):947–957. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
