

The differential diagnosis and treatment of normal-pressure hydrocephalus
- PMID: 22282714
- PMCID: PMC3265984
- DOI: 10.3238/arztebl.2012.0015
The differential diagnosis and treatment of normal-pressure hydrocephalus
Abstract
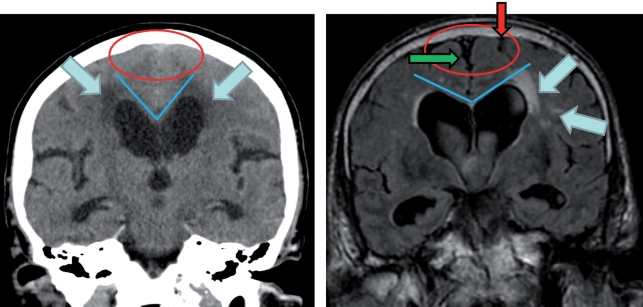
Background: Normal-pressure hydrocephalus (NPH) arises in adulthood and is characterized by a typical combination of clinical and radiological findings. The mean basal intracranial pressure is normal or mildly elevated. The typical signs of the disease are gait impairment, urinary incontinence, and dementia. The difficulty of distinguishing NPH from other neurodegenerative disorders is the likely reason why some 80% of cases remain unrecognized and untreated. According to current evidence, the spontaneous course of NPH ends, for the vast majority of patients, in dependence on nursing care.
Methods: This review article is based on relevant publications retrieved by a selective search in Medline and on national and international guidelines for the management of NPH.
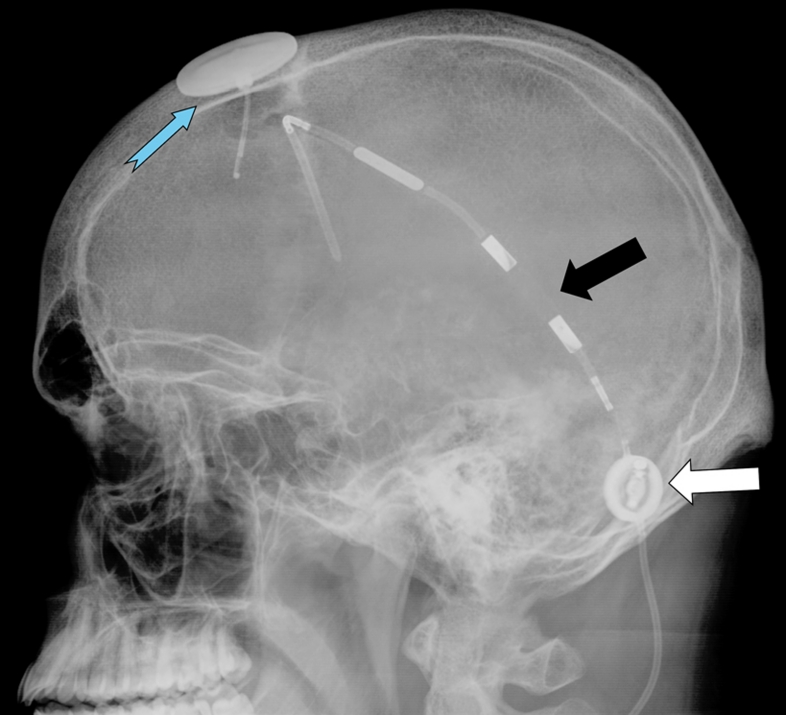
Results: Studies with a high evidence level are lacking; thus, the current state of knowledge about NPH is derived from studies of low or intermediate evidence levels, e.g., observational studies. Modern forms of treatment lead to clinical improvement in 70% to 90% of treated patients. The treatment of choice is the implantation of a ventriculoperitoneal shunt. The differential diagnosis is complicated by the fact that three-quarters of patients with NPH severe enough to require treatment also suffer from another neurodegenerative disorder. Therefore, the clinical findings and imaging studies often do not suffice to establish the indication for surgery. To do this, a further, semi-invasive diagnostic procedure is recommended. Current risk/benefit analyses indicate that shunt operations improve outcome compared to the spontaneous course of the disease.
Conclusion: Normal pressure hydrocephalus should always enter into the differential diagnosis of patients who present with its characteristic manifestations. If the diagnosis of NPH is confirmed, it should be treated at an early stage.
Figures






References
-
- Relkin N, Marmarou A, Klinge P, Bergsneider M, Black PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. 2005;57:4–16. - PubMed
-
- Deutsche Gesellschaft für Neurologie. Leitlinie Normaldruckhydrocephalus. www.dgn.org/images/stories/dgn/leitlinien/LL2008/ll08kap_017.pdf.
-
- Ishikawa M, Hashimoto M, Kuwana N, et al. Guidelines for management of idiopathic normal pressure hydrocephalus. Neurol Med Chir (Tokyo) 2008;48(S1-23) - PubMed
-
- Ziegler U, Doblhammer G. Prevalence and incidence of dementia in Germany—a study based on data from the public sick funds in 2002. Gesundheitswesen. 2009;71:281–290. - PubMed
-
- Brean A, Fredo HL, Sollid S, Muller T, Sundstrom T, Eide PK. Five-year incidence of surgery for idiopathic normal pressure hydrocephalus in Norway. Acta Neurol Scand. 2009;120:314–316. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical