

Intensive care unit-acquired weakness: implications for physical therapist management
- PMID: 22282769
- PMCID: PMC3513482
- DOI: 10.2522/ptj.20110117
Intensive care unit-acquired weakness: implications for physical therapist management
Abstract
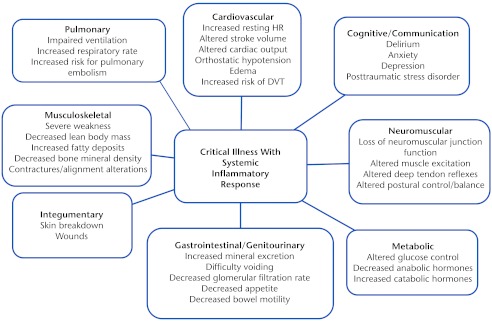
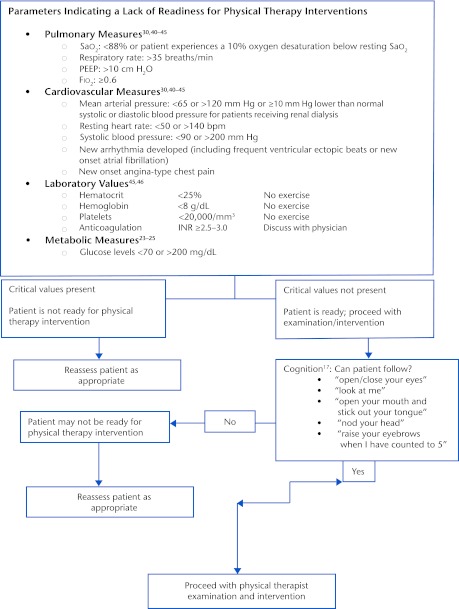
Patients admitted to the intensive care unit (ICU) can develop a condition referred to as "ICU-acquired weakness." This condition is characterized by profound weakness that is greater than might be expected to result from prolonged bed rest. Intensive care unit-acquired weakness often is accompanied by dysfunction of multiple organ systems. Individuals with ICU-acquired weakness typically have significant activity limitations, often requiring physical assistance for even the most basic activities associated with bed mobility. Many of these individuals have activity limitations months to years after hospitalization. The purpose of this article is to review evidence that guides physical rehabilitation of people with ICU-acquired weakness. Included are diagnostic criteria, medical management, and prognostic indicators, as well as criteria for beginning physical rehabilitation, with an emphasis on patient safety. Data are presented indicating that rehabilitation can be implemented with very few adverse effects. Evidence is provided for appropriate measurement approaches and for physical intervention strategies. Finally, some of the key issues are summarized that should be investigated to determine the best intervention guidelines for individuals with ICU-acquired weakness.
Figures
References
-
- Zink W, Kollmar R, Schwab S. Critical illness polyneuropathy and myopathy in the intensive care unit. Nat Rev Neurol. 2009;5:372–379 - PubMed
-
- Bolton CF. Neuromuscular manifestations of critical illness. Muscle Nerve. 2005;32:140–163 - PubMed
-
- Stevens RD, Marshall SA, Cornblath DR, et al. A framework for diagnosing and classifying intensive care unit-acquired weakness. Crit Care Med. 2009;37(10 suppl):S299–S308 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
