

Serum 25-hydroxyvitamin D, transitions between frailty states, and mortality in older adults: the Invecchiare in Chianti Study
- PMID: 22283177
- PMCID: PMC3288698
- DOI: 10.1111/j.1532-5415.2011.03830.x
Serum 25-hydroxyvitamin D, transitions between frailty states, and mortality in older adults: the Invecchiare in Chianti Study
Abstract
Objectives: To assess whether serum 25-hydroxyvitamin D (25(OH)D) concentrations relate to transitions between the states of robustness, prefrailty, and frailty and to mortality in older adults.
Design: The Invecchiare in Chianti (InCHIANTI) Study, a prospective cohort study.
Setting: Tuscany, Italy.
Participants: Adults aged 65 and older (N = 1,155).
Measurements: Serum 25(OH)D concentrations measured at baseline; frailty state (robust, prefrail, frail) assessed at baseline and 3 and 6 years after enrollment; and vital status determined 3 and 6 years after enrollment.
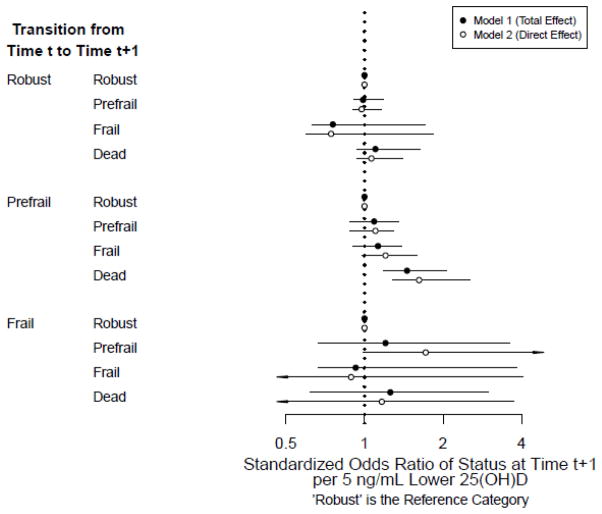
Results: The median (interquartile range) 25(OH)D concentration was 16.0 ng/mL (10.4-25.6 ng/mL; multiply by 2.496 to convert to nmol/L). Prefrail participants with 25(OH)D levels less than 20 ng/mL were 8.9% (95% confidence interval (CI) = 2.5-15.2%) more likely to die, 3.0% (95% CI = -5.6-14.6%) more likely to become frail, and 7.7% (95% CI = -3.5-18.7%) less likely to become robust than prefrail participants with 25(OH)D levels of 20 ng/mL or more. In prefrail participants, each 5-ng/mL decrement of continuous 25(OH)D was associated with 1.46 times higher odds of dying (95% CI = 1.18-2.07) and 1.13 higher odds of incident frailty (95% CI = 0.90-1.39) than with recovery of robustness. Transitions from robustness or frailty were not associated with 25(OH)D levels.
Conclusion: Results provide evidence that prefrailty is an "at risk" state from which older adults with high 25(OH)D levels are more likely to recover than to decline, but high 25(OH)D levels were not associated with recovery from frailty. Thus, 25(OH)D levels should be investigated as a potential therapy to treat prefrailty and prevent further decline.
© 2012, Copyright the Authors Journal compilation © 2012, The American Geriatrics Society.
Conflict of interest statement
Figures
References
-
- Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–156. - PubMed
-
- Fried LP, Ferrucci L, Darer J, et al. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59:255–263. - PubMed
-
- Gill TM, Gahbauer EA, Allore HG, et al. Transitions between frailty states among community-living older persons. Arch Intern Med. 2006;166:418–423. - PubMed
-
- Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev. 2001;22:477–501. - PubMed
-
- Visser M, Deeg DJ, Lips P. Low vitamin D and high parathyroid hormone levels as determinants of loss of muscle strength and muscle mass (sarcopenia): The Longitudinal Aging Study Amsterdam. J Clin Endocrinol Metab. 2003;88:5766–5772. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 AG027012/AG/NIA NIH HHS/United States
- K12 HD043489/HD/NICHD NIH HHS/United States
- T32 AG000262/AG/NIA NIH HHS/United States
- K12HD055931/HD/NICHD NIH HHS/United States
- K12 HD055931/HD/NICHD NIH HHS/United States
- R21 HD057274/HD/NICHD NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- K23AG027746/AG/NIA NIH HHS/United States
- K12HD04389/HD/NICHD NIH HHS/United States
- R21HD057274/HD/NICHD NIH HHS/United States
- K23 AG027746/AG/NIA NIH HHS/United States
- T32 AG00262/AG/NIA NIH HHS/United States
- K25 AG034216/AG/NIA NIH HHS/United States
- R01 HL094507/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
