

Decreased lung hyaluronan in a model of ARDS in the rat: effect of an inhibitor of leukocyte elastase
- PMID: 22283425
- PMCID: PMC3282235
- DOI: 10.3109/03009734.2011.622812
Decreased lung hyaluronan in a model of ARDS in the rat: effect of an inhibitor of leukocyte elastase
Abstract
Background: Hyaluronan (HA) is a component of the extracellular matrix in lung tissue and is normally present at low concentrations in blood. HA is rapidly cleared from blood by the liver. Increased concentrations of plasma HA have been found in patients with acute respiratory distress syndrome (ARDS). We investigated changes in HA levels in plasma, bronchoalveolar lavage fluid (BALF), and lung, and their relationship to pretreatment with a leukocyte elastase inhibitor in a rat model of ARDS.
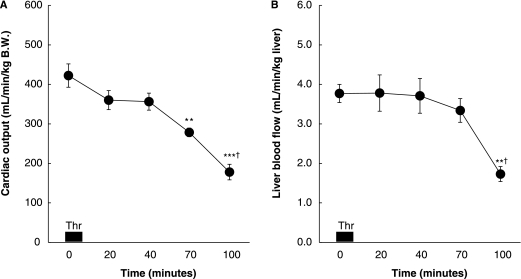
Methods: Rats were randomly assigned to three groups: control, thrombin, and thrombin plus elastase inhibitor. By use of a radiometric assay, HA was measured in lungs, BALF, and plasma. Tissue samples from the lungs were stained for HA and examined microscopically. Liver circulation and cardiac output were monitored using radiolabeled microspheres.
Results: Infusion of thrombin produced a pronounced increase in wet weight to dry weight ratio, and relative lung water content. This increase was blunted by a leukocyte elastase inhibitor. A decrease in lung HA and increases in both BALF and plasma HA were found. The leukocyte elastase inhibitor counteracted not only the decrease in lung tissue HA, but also the increase in plasma HA. Histologically, there was decreased HA-staining of peribronchial and perivascular areas in the injured rat lung. Decreased liver perfusion was observed after infusion of thrombin.
Conclusions: The decrease in lung HA may be involved in the development of pulmonary edema in this ARDS model, and leukocyte elastase may be one cause of this decrease. In addition, an elevated plasma HA level may be an indicator of lung injury.
Figures


References
-
- Quinn DA, Garg HG. Hyaluronan in acute lung injury. In: Vincent JL, editor. Intensive Care Medicine. Annual update 2006. New York: Springer Science + Business Media Inc.; 2006. pp. 349–58. editor. p.
-
- Fraser JRE, Laurent TC, Laurent UBG. Hyaluronan: its nature, distribution, functions and turnover. J Intern Med. 1997;242:27–33. - PubMed
-
- Laurent T. Hyaluronan research in Uppsala. Ups J Med Sci. 2007;112:123–42. - PubMed
-
- Boodoo S, Spannhake EW, Powell JD, Horton MR. Differential regulation of hyaluronan-induced IL-8 and IP-10 in airway epithelial cells. Am J Physiol Lung Cell Mol Physiol. 2006;29:L479–86. - PubMed
-
- Nettelbladt O, Tengblad A, Hällgren R. Accumulation of hyaluronan (hyaluronic acid) in lung tissue during experimental alveolitis parallels development of interstitial edema. Am J Physiol. 1989;257:379–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources