

Risk factors for mortality in smear-negative tuberculosis suspects: a cohort study in Harare, Zimbabwe
- PMID: 22283900
- PMCID: PMC3272461
- DOI: 10.5588/ijtld.11.0056
Risk factors for mortality in smear-negative tuberculosis suspects: a cohort study in Harare, Zimbabwe
Abstract
Objective: To investigate mortality rates and risk factors for death among smear-negative tuberculosis (TB) suspects.
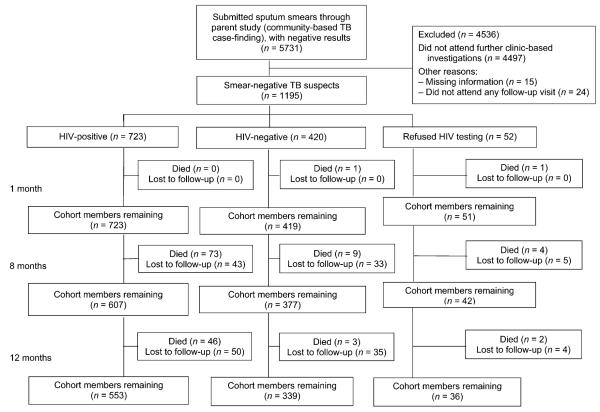
Design: Cohort study nested within a cluster-randomised trial of community-based active case finding. Smear-negative TB suspects were followed for 12 months, with home tracing where necessary. We calculated mortality rates and used regression analysis to investigate the relationship between clinical characteristics and death.
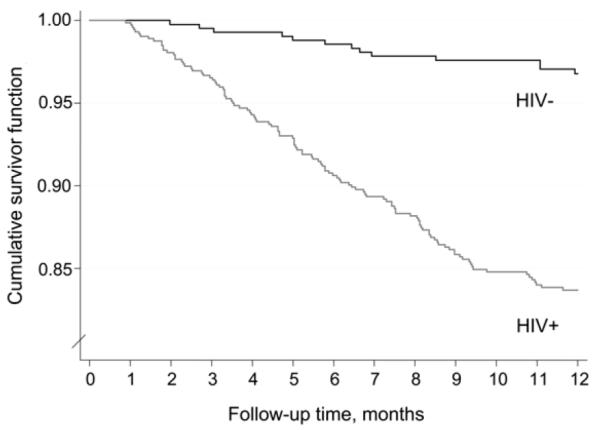
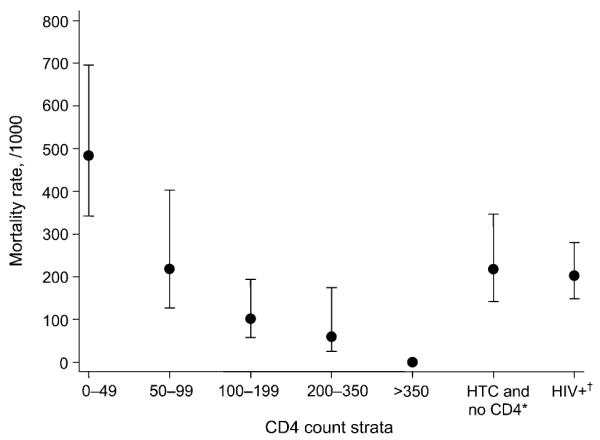
Results: Between February 2006 and June 2007, 1195 smear-negative TB suspects were followed for 1136.8 person-years. Human immunodeficiency virus (HIV) prevalence was 63.3%. During follow-up, 139 participants died (11.6%) and mortality rates remained high throughout; 119 (16.5%) HIV-positive individuals and 13 (3.1%) HIV-negative individuals died (HR = 5.8, 95%CI 3.3-10.4, P < 0.001). Advanced immunosuppression was the main risk factor for death among HIV-positive participants, with CD4 count < 50 cells/μ l associated with a 13-fold increased risk of death. Antiretroviral treatment (ART) was initiated by only 106 (14.7%), with long delays in accessing care.
Conclusion: HIV-positive smear-negative TB suspects are at high and sustained risk of death. Current guidelines for the management of HIV-infected TB suspects are limited, and this study adds to evidence that specific policies are required to promote earlier HIV and TB diagnosis and reduce delays in ART initiation.
Figures
References
-
- Joint United Nations Programme on HIV/AIDS . AIDS epidemic update. UNAIDS; Geneva, Switzerland: 2009.
-
- World Health Organization . Global tuberculosis control: epidemiology, strategy, financing. WHO; Geneva, Switzerland: 2009. WHO/HTM/TB/2009.411.
-
- Corbett EL, Marston B, Churchyard GJ, De Cock KM. Tuberculosis in sub-Saharan Africa: opportunities, challenges and change in the era of antiretroviral treatment. Lancet. 2006;367:926–937. - PubMed
-
- Stop TB Partnership . The global plan to stop TB, 2006–2015. WHO; Geneva, Switzerland: 2006.
-
- Marais BJ, Raviglione MC, Donald PR, et al. Scale-up of services and research priorities for diagnosis, management, and control of tuberculosis: a call to action. Lancet. 2010;375:2179–2191. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
