

Predictors of survival in a cohort of patients with polymyositis and dermatomyositis: effect of corticosteroids, methotrexate and azathioprine
- PMID: 22284862
- PMCID: PMC3392815
- DOI: 10.1186/ar3704
Predictors of survival in a cohort of patients with polymyositis and dermatomyositis: effect of corticosteroids, methotrexate and azathioprine
Abstract
Introduction: The idiopathic inflammatory myopathies are rare diseases for which data regarding the natural history, response to therapies and factors affecting mortality are needed. We performed this study to examine the effects of treatment and clinical features on survival in polymyositis and dermatomyositis patients.
Methods: A total of 160 consecutive patients (77 with polymyositis and 83 with dermatomyositis) seen at the University of Michigan from 1997 to 2003 were included. Medical records were abstracted for clinical, laboratory and therapeutic data, including initial steroid regimen and immunosuppressive use. State vital records were utilized to derive mortality and cause of death data. Survival was modeled by left-truncated Kaplan-Meier estimation and Cox regression.
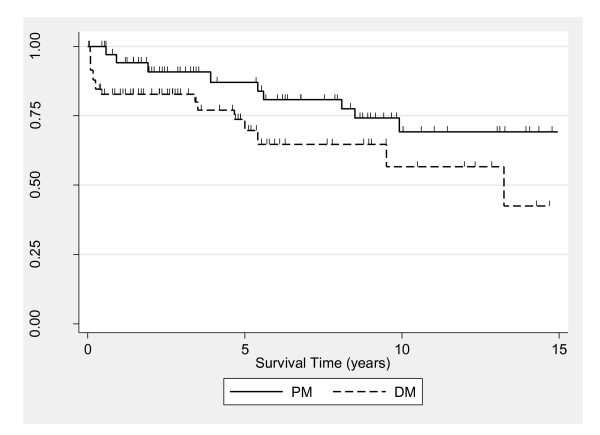
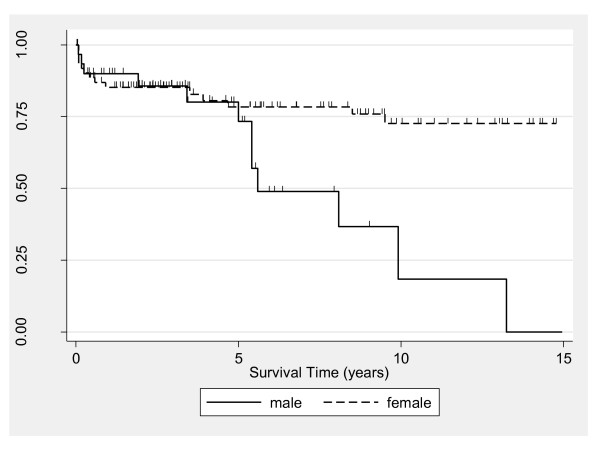
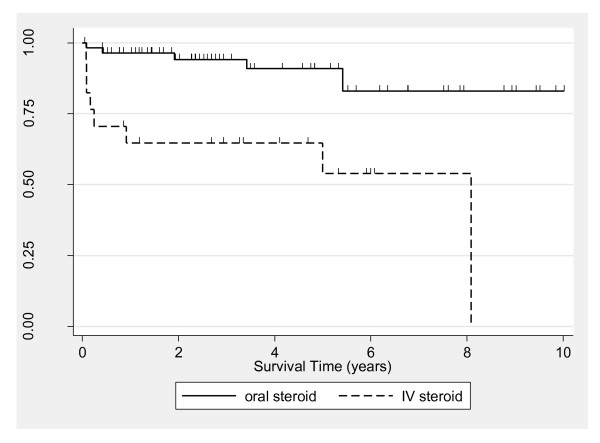
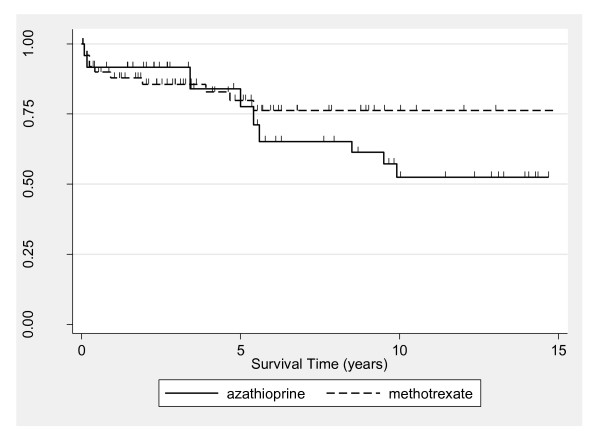
Results: The 5- and 10-year survival estimates were 77% (95% CI = 66 to 85), and 62% (95% CI = 48 to 73), respectively, and the rates were similar for polymyositis and dermatomyositis. Survival between the sexes was similar through 5 years and significantly lower thereafter for males (10-year survival: 18% male, 73% female; P = 0.002 for 5- to 10-year interval). The sex disparity was restricted to the polymyositis group. Increased age at diagnosis and non-Caucasian race were associated with lower survival. Intravenous versus oral corticosteroid use was associated with a higher risk of death among Caucasians (HR = 10.6, 95% CI = 2.1 to 52.8). Early survival between patients treated with methotrexate versus azathioprine was similar, but survival at 10 years was higher for the methotrexate-treated group (76% vs 52%, P = 0.046 for 5- to 10-year interval).
Conclusions: Patients treated initially with intravenous corticosteroids had higher mortality, which was likely related to disease severity. Both methotrexate and azathioprine showed similar early survival benefits as first-line immunosuppressive drugs. Survival was higher between 5 and 10 years in the methotrexate-treated group, but could not be confirmed in multivariable modeling for the full follow-up period. Other important predictors of long-term survival included younger age, female sex and Caucasian race.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
