

Stereotactic body radiation therapy for management of spinal metastases in patients without spinal cord compression: a phase 1-2 trial
- PMID: 22285199
- PMCID: PMC3605896
- DOI: 10.1016/S1470-2045(11)70384-9
Stereotactic body radiation therapy for management of spinal metastases in patients without spinal cord compression: a phase 1-2 trial
Abstract
Background: Spinal stereotactic body radiation therapy (SBRT) is increasingly used to manage spinal metastases, yet the technique's effectiveness in controlling the symptom burden of spinal metastases has not been well described. We investigated the clinical benefit of SBRT for managing spinal metastases and reducing cancer-related symptoms.
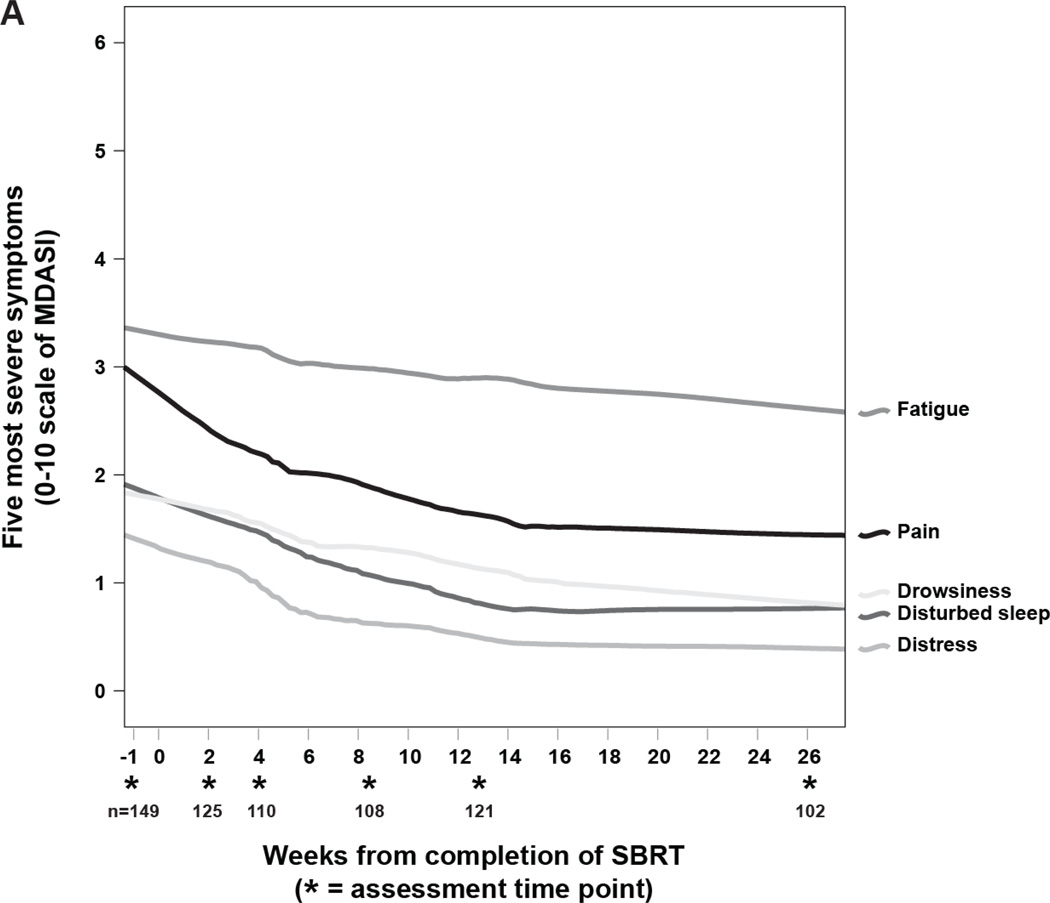
Methods: 149 patients with mechanically stable, non-cord-compressing spinal metastases (166 lesions) were given SBRT in a phase 1-2 study. Patients received a total dose of 27-30 Gy, typically in three fractions. Symptoms were measured before SBRT and at several time points up to 6 months after treatment, by the Brief Pain Inventory (BPI) and the M D Anderson Symptom Inventory (MDASI). The primary endpoint was frequency and duration of complete pain relief. The study is completed and is registered with ClinicalTrials.gov, number NCT00508443.
Findings: Median follow-up was 15·9 months (IQR 9·5-30·3). The number of patients reporting no pain from bone metastases, as measured by the BPI, increased from 39 of 149 (26%) before SBRT to 55 of 102 (54%) 6 months after SBRT (p<0·0001). BPI-reported pain reduction from baseline to 4 weeks after SBRT was clinically meaningful (mean 3·4 [SD 2·9] on the BPI pain-at-its-worst item at baseline, 2·1 [2·4] at 4 weeks; effect size 0·47, p=0·00076). These improvements were accompanied by significant reduction in opioid use during the first 6 months after SBRT (43 [28·9%] of 149 patients with strong opioid use at baseline vs 20 [20·0%] of 100 at 6 months; p=0·011). Ordinal regression modelling showed that patients reported significant pain reduction according to the MDASI during the first 6 months after SBRT (p=0·00003), and significant reductions in a composite score of the six MDASI symptom interference with daily life items (p=0·0066). Only a few instances of non-neurological grade 3 toxicities occurred: nausea (one event), vomiting (one), diarrhoea (one), fatigue (one), dysphagia (one), neck pain (one), and diaphoresis (one); pain associated with severe tongue oedema and trismus occurred twice; and non-cardiac chest pain was reported three times. No grade 4 toxicities occurred. Progression-free survival after SBRT was 80·5% (95% CI 72·9-86·1) at 1 year and 72·4% (63·1-79·7) at 2 years.
Interpretation: SBRT is an effective primary or salvage treatment for mechanically stable spinal metastasis. Significant reductions in patient-reported pain and other symptoms were evident 6 months after SBRT, along with satisfactory progression-free survival and no late spinal cord toxicities.
Funding: National Cancer Institute of the US National Institutes of Health.
Copyright © 2012 Elsevier Ltd. All rights reserved.
Conflict of interest statement
LDR has received teaching honoraria from Medtronic and Stryker. The remaining authors declare no conflicts of interest. The corresponding author states that she had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Figures


Comment in
-
SBRT and spinal metastasis: finding its niche.Lancet Oncol. 2012 Apr;13(4):328-9. doi: 10.1016/S1470-2045(12)70002-5. Epub 2012 Jan 27. Lancet Oncol. 2012. PMID: 22285200 No abstract available.
References
-
- Klimo P, Jr, Kestle JR, Schmidt MH. Clinical trials and evidence-based medicine for metastatic spine disease. Neurosurg Clin N Am. 2004;15:549–564. - PubMed
-
- Chang EL, Shiu AS, Mendel E, et al. Phase I/II study of stereotactic body radiotherapy for spinal metastasis and its pattern of failure. J Neurosurg Spine. 2007;7:151–160. - PubMed
-
- Gagnon GJ, Nasr NM, Liao JJ, et al. Treatment of spinal tumors using cyberknife fractionated stereotactic radiosurgery: pain and quality-of-life assessment after treatment in 200 patients. Neurosurgery. 2009;64:297–306. - PubMed
-
- Janjan NA, Payne R, Gillis T, et al. Presenting symptoms in patients referred to a multidisciplinary clinic for bone metastases. J Pain Symptom Manage. 1998;16:171–178. - PubMed
-
- Prasad D, Schiff D. Malignant spinal-cord compression. Lancet Oncol. 2005;6:15–24. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
