

Resolution of acute pain following discharge from the emergency department: the acute pain trajectory
- PMID: 22285610
- PMCID: PMC3294147
- DOI: 10.1016/j.jpain.2011.11.007
Resolution of acute pain following discharge from the emergency department: the acute pain trajectory
Abstract
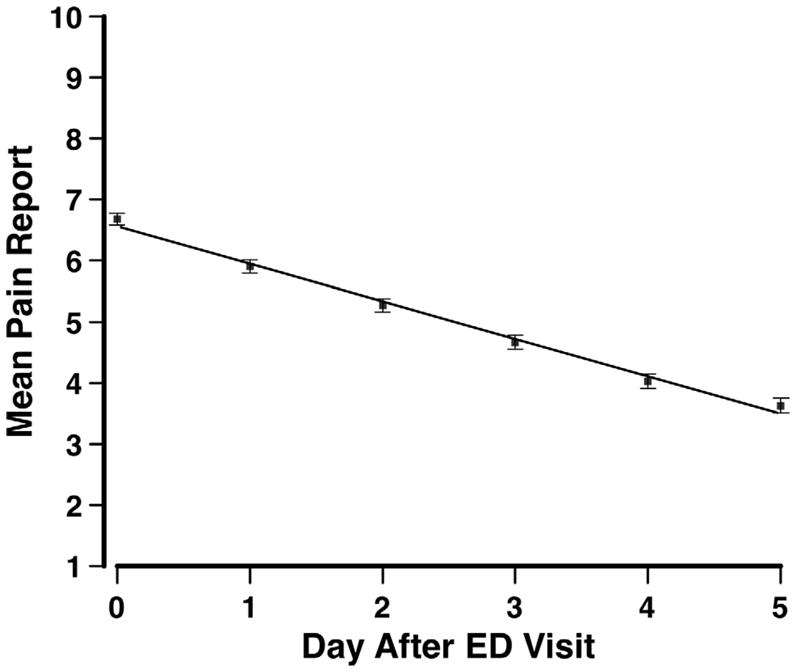
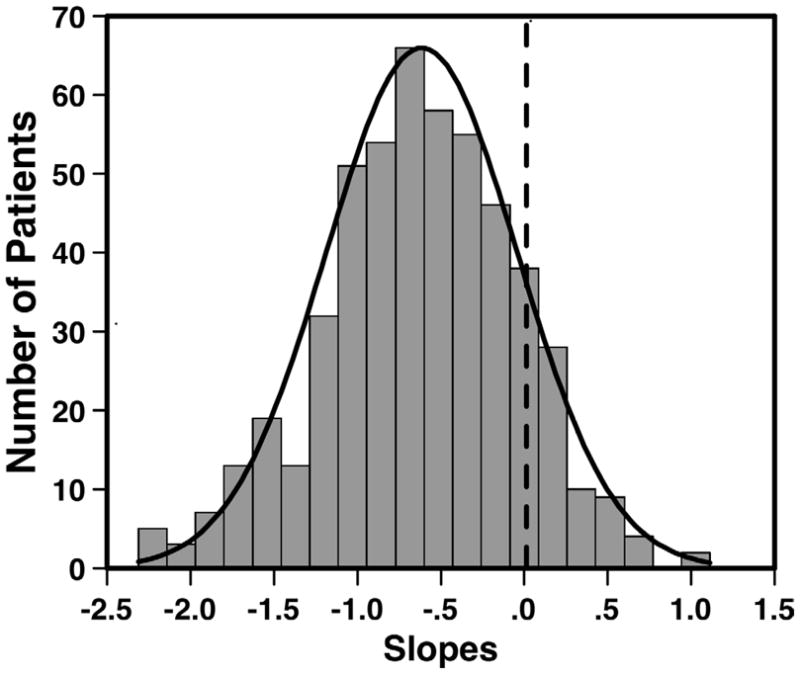
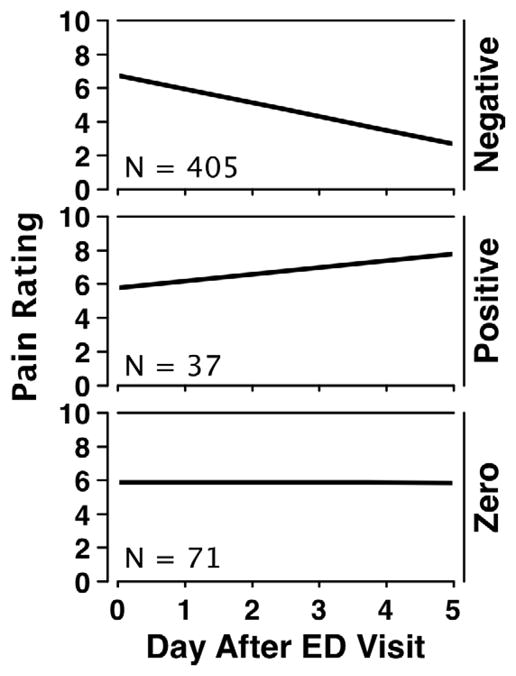
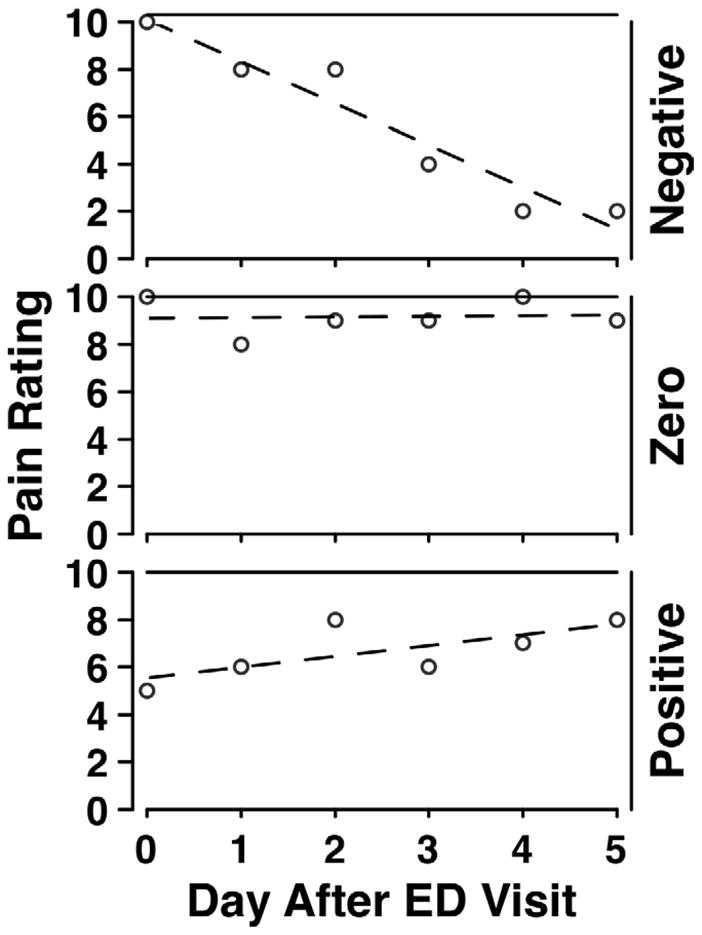
We demonstrate and evaluate a method for modeling acute pain resolution in individual patients over 6 days following an emergency department visit for an acutely painful condition. Five hundred and thirteen patients presenting with acutely painful conditions provided 11-point numerical ratings of pain intensity at discharge from an emergency department and daily thereafter for a total of 6 days. Latent growth curve modeling with a linear fit yielded measures of initial pain intensity (intercept) and rate of pain resolution (slope) for each individual patient. The linear fits provided good approximations of individual pain trajectories. The average patient had intercept of 6.57 with a slope of -.61. On Day 4, 54.6% of patients reported a pain level equal to or greater than 4. Classification of individual patients by slope revealed that 79% of the sample had the expected negative slope for acute pain resolution while 21% had flat or positive slopes, indicating lack of pain resolution or worsening of pain over time following discharge. The standard errors of measurement for the acute pain trajectories were markedly smaller than those for conventional pain ratings, indicating that the trajectory approach to pain measurement improves measurement precision.
Perspective: The acute pain trajectory provides more information than conventional pain measurement and increases measurement precision. It provides a means of determining the efficacy of acute pain management in the emergency department. The rate of pain resolution is a potentially valuable outcome measure for controlled clinical trials.
Copyright © 2012 American Pain Society. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors have no financial or other relationships that constitute a conflict of interest.
Figures
References
-
- Johnston CC, Gagnon AJ, Pepler CJ, Bourgault P. Pain in the emergency department with one-week follow-up of pain resolution. Pain Res Manag. 2005;10:67–70. - PubMed
-
- Rupp T, Delaney KA. Inadequate analgesia in emergency medicine. Ann Emerg Med. 2004;43:494–503. - PubMed
-
- Todd KH, Ducharme J, Choiniere M, Crandall CS, Fosnocht DE, Homel P, Tanabe P PEMI Study Group. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007;8:460–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
