

Amyloid imaging in dementias with atypical presentation
- PMID: 22285638
- PMCID: PMC3517915
- DOI: 10.1016/j.jalz.2011.07.003
Amyloid imaging in dementias with atypical presentation
Abstract
Background: With the potential emergence of disease specific therapies, an accurate biomarker of Alzheimer's Disease pathology is needed in cases in which the underlying etiology is uncertain. We explored the potential value of amyloid imaging in patients with atypical presentations of dementia.
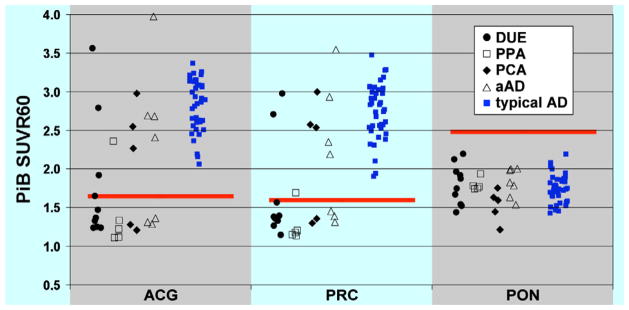
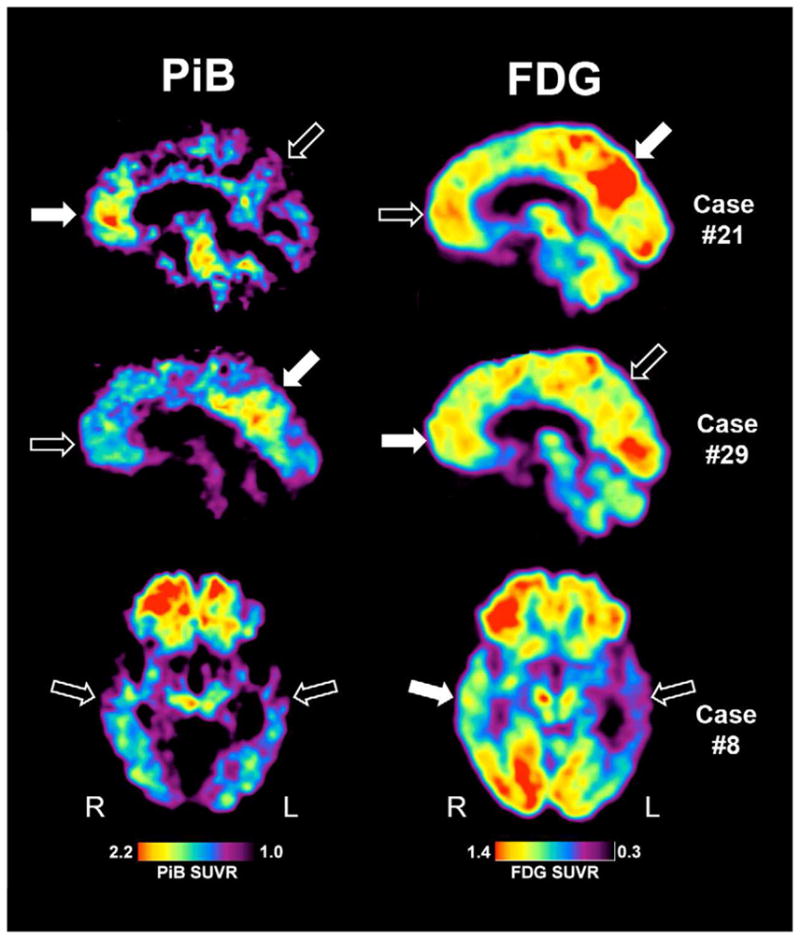
Methods: Twenty-eight patients with atypical dementia underwent positron emission tomography imaging with the amyloid imaging tracer Pittsburgh compound B (PiB). Twenty-six had [18F]fluoro-2-deoxy-D-glucose positron emission tomography scans. After extensive clinical evaluation, this group of patients generated considerable diagnostic uncertainty and received working diagnoses that included possible Alzheimer's disease (AD), focal dementias (e.g., posterior cortical atrophy [PCA]), or cases in which no clear diagnostic category could be determined (dementia of uncertain etiology). Patients were classified as PiB-positive, PiB-negative, or PiB-intermediate, based on objective criteria. Anterior-posterior and left-right indices of PiB and [18F]fluoro-2-deoxy-D-glucose uptake were calculated to examine differences in distribution of amyloid pathology and metabolic changes associated with clinical phenotype.
Results: Eleven patients (39%) were PiB positive, 16 were PiB negative (57%), and one (4%) was PiB intermediate. By diagnostic category, three of 10 patients (30%) with dementia of uncertain etiology, one of five (20%) with primary progressive aphasia, three of five (60%) with PCA, and four of seven (57%) with possible AD were PiB positive. Brain metabolism of both PiB-positive and PiB-negative patients was generally similar by phenotype, but appeared to differ from typical AD. PCA patients also appeared to differ in their relative distribution of PiB compared with typical AD, consistent with their atypical phenotype.
Conclusions: AD pathology is frequently present in atypical presentations of dementia and can be identified by amyloid imaging. Clinical phenotype is more related to the pattern of cerebral hypometabolism than the presence/absence of amyloid pathology. These findings have diagnostic, prognostic, and therapeutic implications.
Copyright © 2012 The Alzheimer's Association. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment--beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–6. - PubMed
-
- Petersen RC. Mild cognitive impairment as a diagnostic entity. Journal of Internal Medicine. 2004;256:183–94. - PubMed
-
- Alladi S, Xuereb J, Bak T, et al. Focal cortical presentations of Alzheimer’s disease. Brain. 2007;130:2636–45. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
