

Resting heart rate and the risk of death and cardiovascular complications in patients with type 2 diabetes mellitus
- PMID: 22286552
- PMCID: PMC4170780
- DOI: 10.1007/s00125-012-2471-y
Resting heart rate and the risk of death and cardiovascular complications in patients with type 2 diabetes mellitus
Abstract
Aims/hypothesis: An association between resting heart rate and mortality has been described in the general population and in patients with cardiovascular disease. There are, however, few data exploring this relationship in patients with type 2 diabetes mellitus. The current study addresses this issue.
Methods: The relationship between baseline resting heart rate and all-cause mortality, cardiovascular death and major cardiovascular events (cardiovascular death, non-fatal myocardial infarction or non-fatal stroke) was examined in 11,140 patients who participated in the Action in Diabetes and Vascular Disease: Preterax and Diamicron Modified Release Controlled Evaluation (ADVANCE) Study.
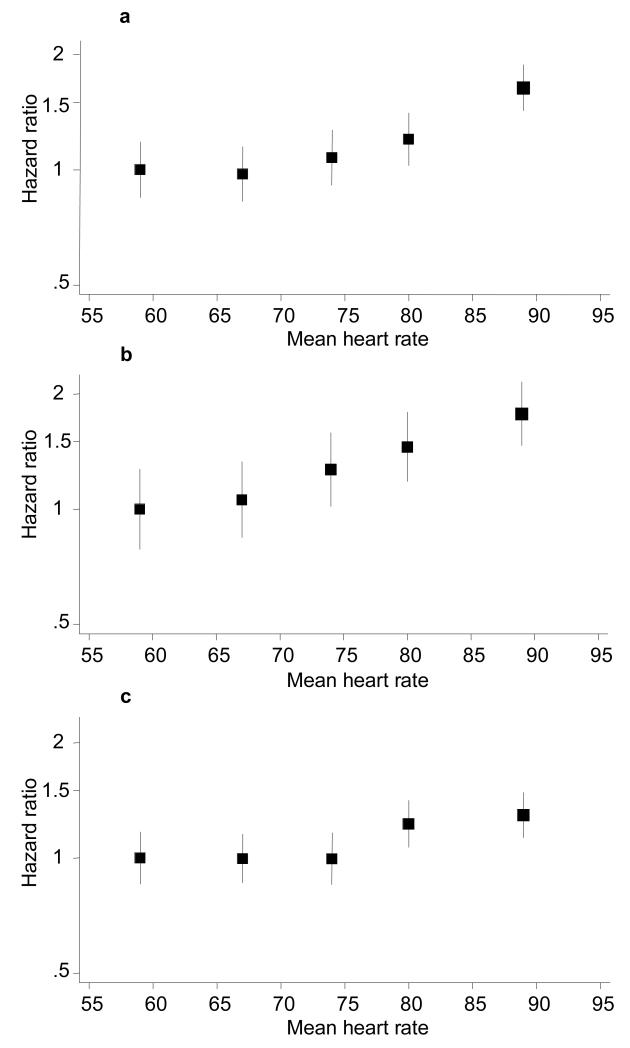
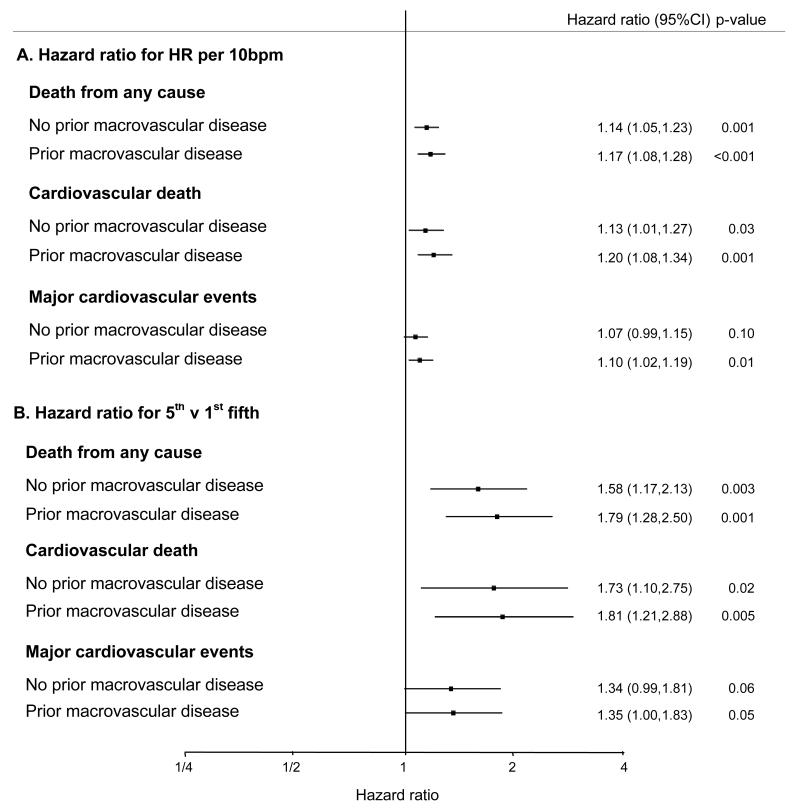
Results: A higher resting heart rate was associated with a significantly increased risk of all-cause mortality (fully adjusted HR 1.15 per 10 bpm [95% CI 1.08, 1.21], p<0.001), cardiovascular death and major cardiovascular outcomes without adjustment and after adjusting for age and sex and multiple covariates. The increased risk associated with a higher baseline resting heart rate was most obvious in patients with previous macrovascular complications (fully adjusted HR for death 1.79 for upper [mean 91 bpm] vs lowest [mean 58 bpm] fifth of resting heart rate in this subgroup [95% CI 1.28, 2.50], p = .001).
Conclusions/interpretation: Among patients with type 2 diabetes, a higher resting heart rate is associated with an increased risk of death and cardiovascular complications. It remains unclear whether a higher heart rate directly mediates the increased risk or is a marker for other factors that determine a poor outcome.
Figures
References
-
- Fox K, Borer JS, Camm AJ, et al. Resting heart rate in cardiovascular disease. J Am Coll Cardiol. 2007;50:823–830. - PubMed
-
- Palatini P. Elevated heart rate in cardiovascular diseases: a target for treatment? Prog Cardiovasc Dis. 2009;52:46–60. - PubMed
-
- Patel A, MacMahon S, Chalmers J, et al. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet. 2007;370:829–840. - PubMed
-
- Patel A, MacMahon S, Chalmers J, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358:2560–2572. - PubMed
-
- ADVANCE study group Study rationale and design of ADVANCE: action in diabetes and vascular disease--preterax and diamicron MR controlled evaluation. Diabetologia. 2001;44:1118–1120. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
