

Comparison of wideband steady-state free precession and T₂-weighted fast spin echo in spine disorder assessment at 1.5 and 3 T
- PMID: 22287191
- PMCID: PMC3712341
- DOI: 10.1002/mrm.24163
Comparison of wideband steady-state free precession and T₂-weighted fast spin echo in spine disorder assessment at 1.5 and 3 T
Abstract
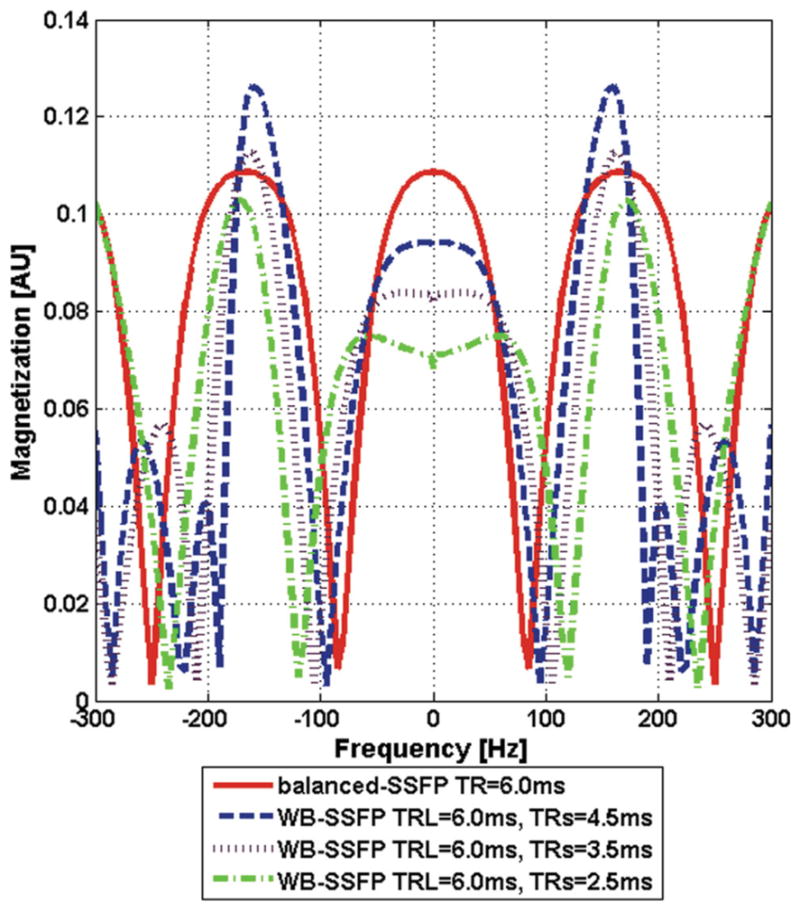
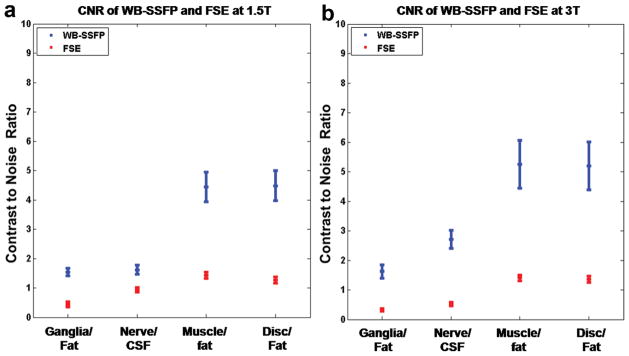
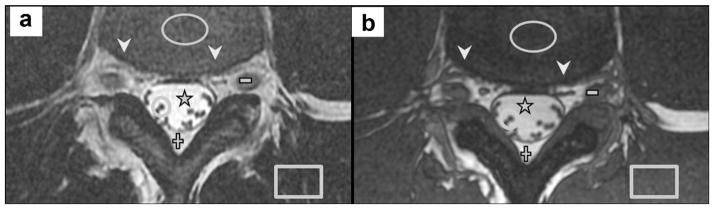
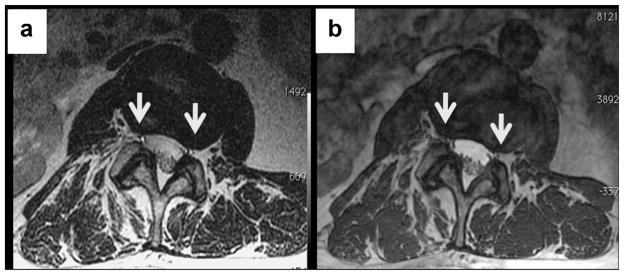
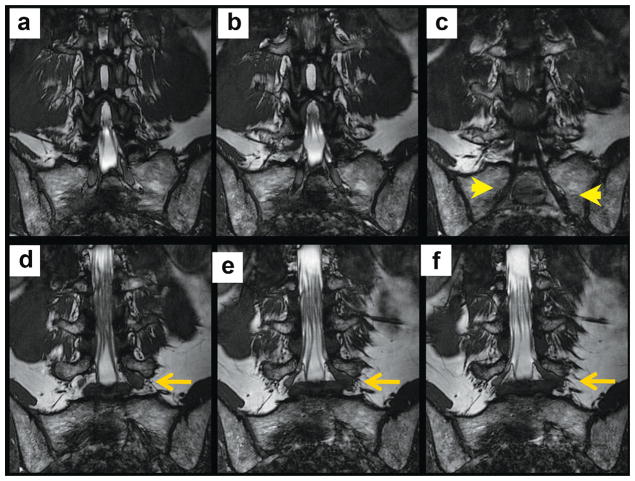
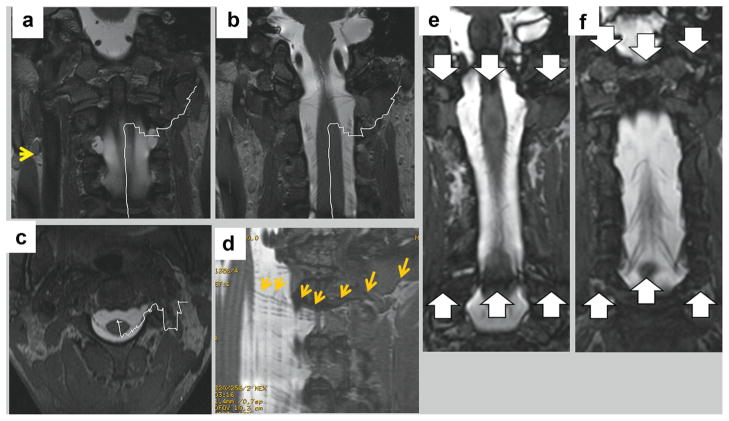
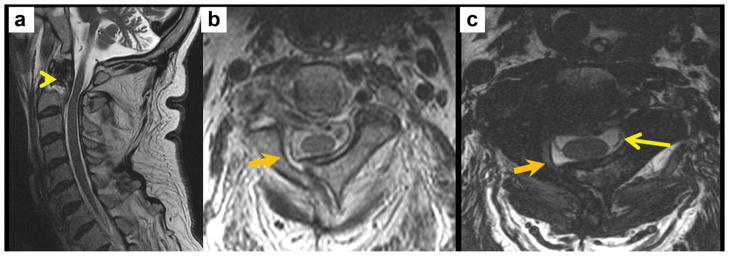
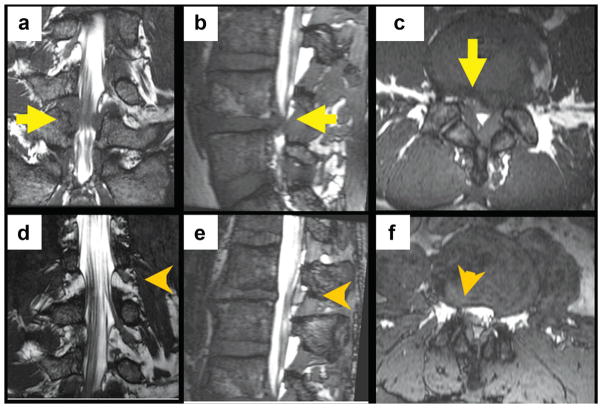
Wideband steady-state free precession (WB-SSFP) is a modification of balanced steady-state free precession utilizing alternating repetition times to reduce susceptibility-induced balanced steady-state free precession limitations, allowing its use for high-resolution myelographic-contrast spinal imaging. Intertissue contrast and spatial resolution of complete-spine-coverage 3D WB-SSFP were compared with those of 2D T₂-weighted fast spin echo, currently the standard for spine T₂-imaging. Six normal subjects were imaged at 1.5 and 3 T. The signal-to-noise ratio efficiency (SNR per unit-time and unit-volume) of several tissues was measured, along with four intertissue contrast-to-noise ratios; nerve-ganglia:fat, intradural-nerves:cerebrospinal fluid, nerve-ganglia:muscle, and muscle:fat. Patients with degenerative and traumatic spine disorders were imaged at both MRI fields to demonstrate WB-SSFP clinical advantages and disadvantages. At 3 T, WB-SSFP provided spinal contrast-to-noise ratios 3.7-5.2 times that of fast spin echo. At 1.5 T, WB-SSFP contrast-to-noise ratio was 3-3.5 times that of fast spin echo, excluding a 1.7 ratio for intradural-nerves:cerebrospinal fluid. WB-SSFP signal-to-noise ratio efficiency was also higher. Three-dimensional WB-SSFP disadvantages relative to 2D fast spin echo are reduced edema hyperintensity, reduced muscle signal, and higher motion sensitivity. WB-SSFP's high resolution and contrast-to-noise ratio improved visualization of intradural nerve bundles, foraminal nerve roots, and extradural nerve bundles, improving detection of nerve compression in radiculopathy and spinal-stenosis. WB-SSFP's high resolution permitted reformatting into orthogonal planes, providing distinct advantages in gauging fine spine pathology.
Copyright © 2012 Wiley Periodicals, Inc.
Figures
References
-
- Grams AE, Gempt J, Forschler A. Comparison of spinal anatomy between 3-Tesla MRI and CT-myelography under healthy and pathological conditions. Surg Radiol Anat. 2010;32:581. - PubMed
-
- Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. N Engl J Med. 2008;358:818–825. - PubMed
-
- Rubinstein SM, van Tulder M. A best-evidence review of diagnostic procedures for neck and low-back pain. Best Pract Res Clin Rheumatol. 2008;22:471–482. - PubMed
-
- Rathmell JP. A 50-year-old man with chronic low back pain. JAMA. 2008;299:2066–2077. - PubMed
-
- Bono CM, Ghiselli G, Gilbert TJ, Kreiner DS, Reitman C, Summers JT, Baisden JL, Easa J, Fernand R, Lamer T, Matz PG, Mazanec DJ, Resnick DK, Shaffer WO, Sharma AK, Timmons RB, Toton JF North American Spine Society. An evidence-based clinical guideline for the diagnosis and treatment of cervical radiculopathy from degenerative disorders. Spine J. 2011;11:64–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
