

Induction of MAGE-A3 and HPV-16 immunity by Trojan vaccines in patients with head and neck carcinoma
- PMID: 22287423
- PMCID: PMC3725741
- DOI: 10.1002/hed.22004
Induction of MAGE-A3 and HPV-16 immunity by Trojan vaccines in patients with head and neck carcinoma
Abstract
Background: We performed a pilot study using Trojan vaccines in patients with advanced squamous cell carcinoma of the head and neck (SCCHN). These vaccines are composed of HLA-I and HLA-II restricted melanoma antigen E (MAGE)-A3 or human papillomavirus (HPV)-16 derived peptides, joined by furin-cleavable linkers, and linked to a "penetrin" peptide sequence derived from HIV-TAT. Thirty-one patients with SCCHN were screened for the trial and 5 were enrolled.
Methods: Enrolled patients were treated with 300 μg of Trojan peptide supplemented with Montanide and granulocyte-macrophage colony-stimulating factor (GM-CSF) at 4-week intervals for up to 4 injections.
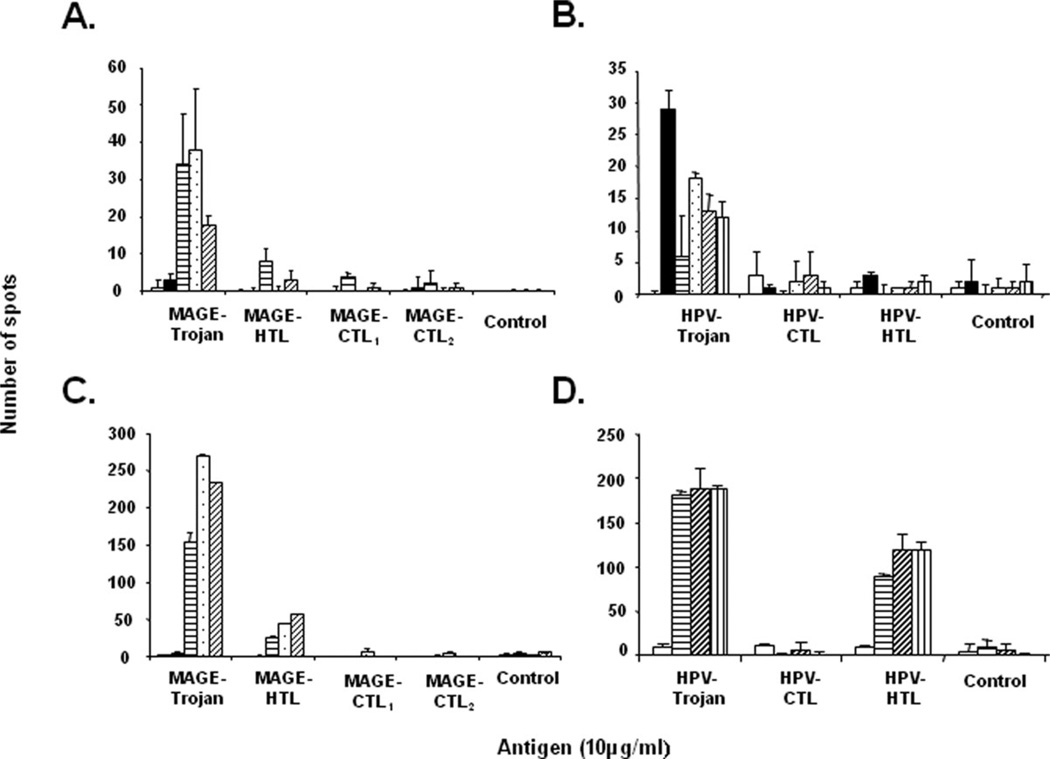
Results: Following vaccination, peripheral blood mononuclear cells (PBMCs) from 4 of 5 patients recognized both the full Trojan constructs and constituent HLA-II peptides, whereas responses to HLA-I restricted peptides were less pronounced.
Conclusion: This treatment regimen seems to have acceptable toxicity and elicits measurable systemic immune responses against HLA-II restricted epitopes in a subset of patients with advanced SCCHN.
Copyright © 2012 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of interest: Dr. Strome is a major stockholder in Gliknik, a biotechnology company. Gliknik has licensed the rights to this vaccine technology from the University of Maryland. Dr. Strome receives royalties from the licensure of this technology. Dr. Celis receives royalties from the Mayo Clinic College of Medicine as an inventor of the Trojan peptide vaccines.
Figures





References
-
- Ahmed SM, Cohen EE. Treatment of squamous cell carcinoma of the head and neck in the metastatic and refractory settings: advances in chemotherapy and the emergence of small molecule epidermal growth factor receptor kinase inhibitors. Curr Cancer Drug Targets. 2007;7:666–673. - PubMed
-
- Voskens CJ, Strome SE, Sewell DA. Synthetic peptide-based cancer vaccines: lessons learned and hurdles to overcome. Curr Mol Med. 2009;9:683–693. - PubMed
-
- Zwaveling S, Ferreira Mota SC, Nouta J, et al. Established human papillomavirus type 16-expressing tumors are effectively eradicated following vaccination with long peptides. J Immunol. 2002;169:350–358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
