

Position of probe determines prognostic information of brain tissue PO2 in severe traumatic brain injury
- PMID: 22289784
- PMCID: PMC3954543
- DOI: 10.1227/NEU.0b013e31824ce933
Position of probe determines prognostic information of brain tissue PO2 in severe traumatic brain injury
Abstract
Background: Monitoring brain tissue PO2 (PbtO2) is part of multimodality monitoring of patients with traumatic brain injury (TBI). However, PbtO2 measurement is a sampling of only a small area of tissue surrounding the sensor tip.
Objective: To examine the effect of catheter location on the relationship between PbtO2 and neurological outcome.
Methods: A total of 405 patients who had PbtO2 monitoring as part of standard management of severe traumatic brain injury were studied. The relationships between probe location and resulting PbtO2 and outcome were examined.
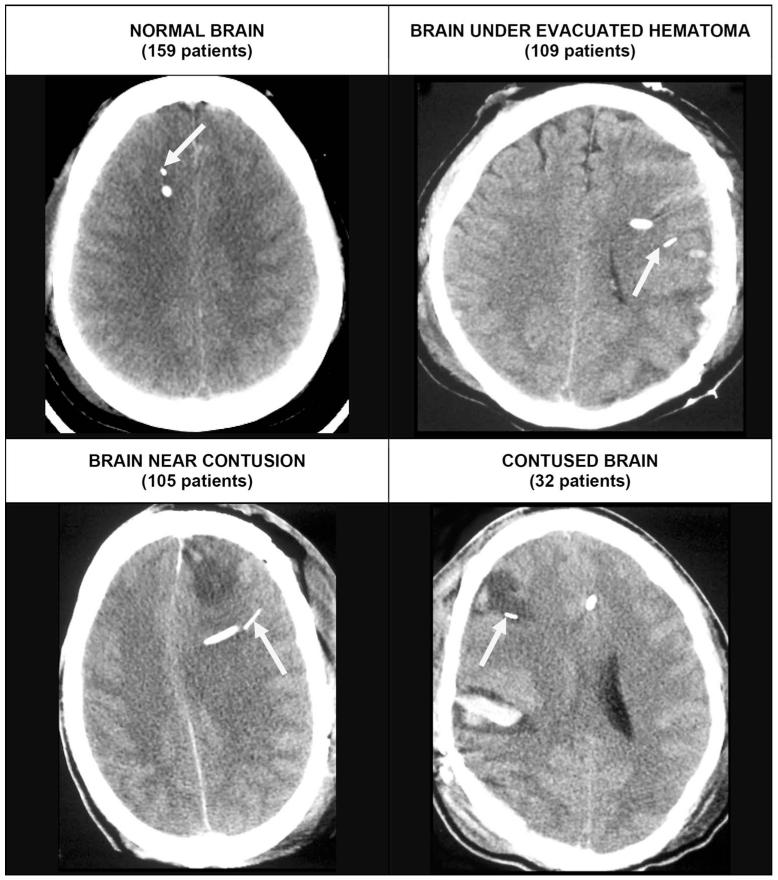
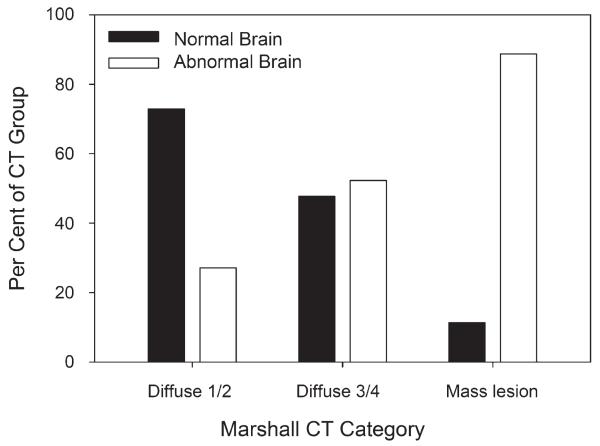
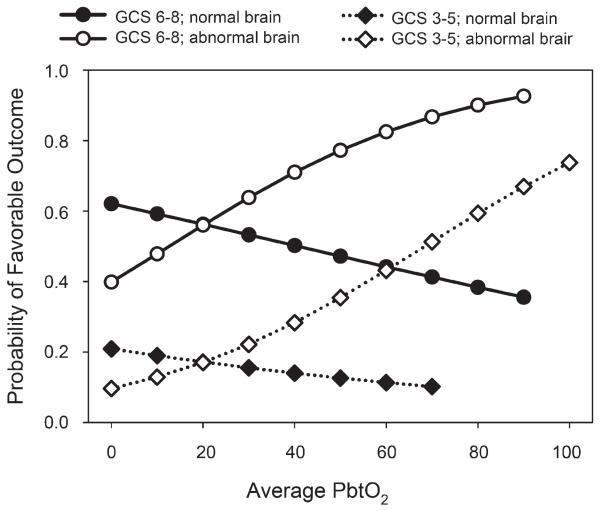
Results: When the probe was located in normal brain, PbtO2 averaged 30.8 ± 18.2 compared with 25.6 ± 14.8 mm Hg when placed in abnormal brain (P < .001). Factors related to neurological outcome in the best-fit logistic regression model were age, PbtO2 probe position, postresuscitation motor Glasgow Coma Scale score, and PbtO2 trend pattern. Although average PbtO2 was significantly related to outcome in univariate analyses, it was not significant in the final logistic model. However, the interaction between PbtO2 and probe position was statistically significant. When the PbtO2 probe was placed in abnormal brain, the average PbtO2 was higher in those with a favorable outcome, 28.8 ± 12.0 mm Hg, compared with those with an unfavorable outcome, 19.5 ± 13.7 mm Hg (P = .01). PbtO2 and outcome were not related when the probe was placed in normal-appearing brain.
Conclusion: These results suggest that the location of the PbtO2 probe determines the PbtO2 values and the relationship of PbtO2 to neurological outcome.
Figures

References
-
- Bratton SL, Chestnut RM, Ghajar J, et al. Guidelines for the management of severe traumatic brain injury, X: rain oxygen monitoring and thresholds. J Neurotrauma. 2007;24(suppl 1):S65–S70. - PubMed
-
- De Georgia MA, Deogaonkar A. Multimodal monitoring in the neurological intensive care unit. Neurologist. 2005;11(1):45–54. - PubMed
-
- Wartenberg KE, Schmidt JM, Mayer SA. Multimodality monitoring in neurocritical care. Crit Care Clin. 2007;23(3):507–538. - PubMed
-
- Stiefel MF, Spiotta A, Gracias VH, et al. Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring. J Neurosurg. 2005;103(5):805–811. - PubMed
-
- Narotam PK, Morrison JF, Nathoo N. Brain tissue oxygen monitoring in traumatic brain injury and major trauma: outcome analysis of a brain tissue oxygen-directed therapy. J Neurosurg. 2009;111(4):672–682. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
