

Potassium-channel mutations and cardiac arrhythmias--diagnosis and therapy
- PMID: 22290238
- PMCID: PMC6590894
- DOI: 10.1038/nrcardio.2012.3
Potassium-channel mutations and cardiac arrhythmias--diagnosis and therapy
Abstract
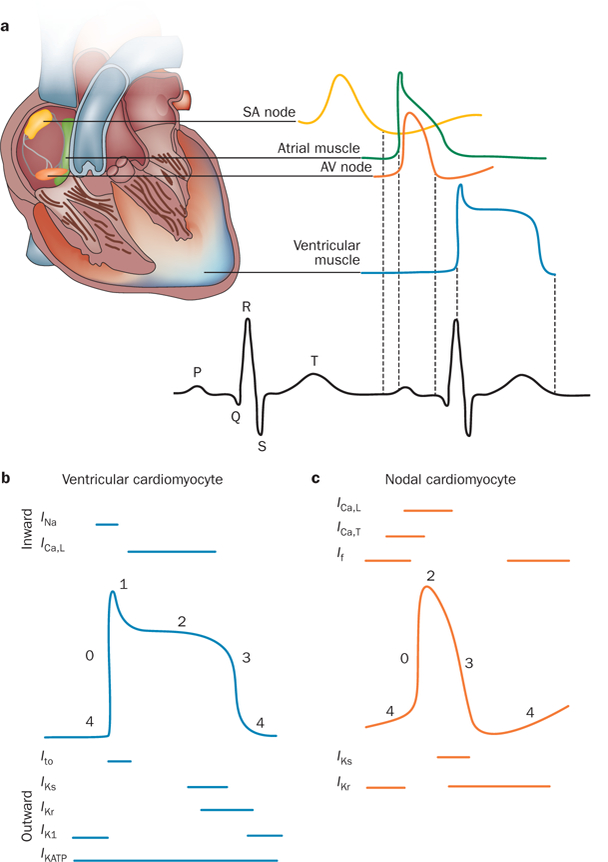
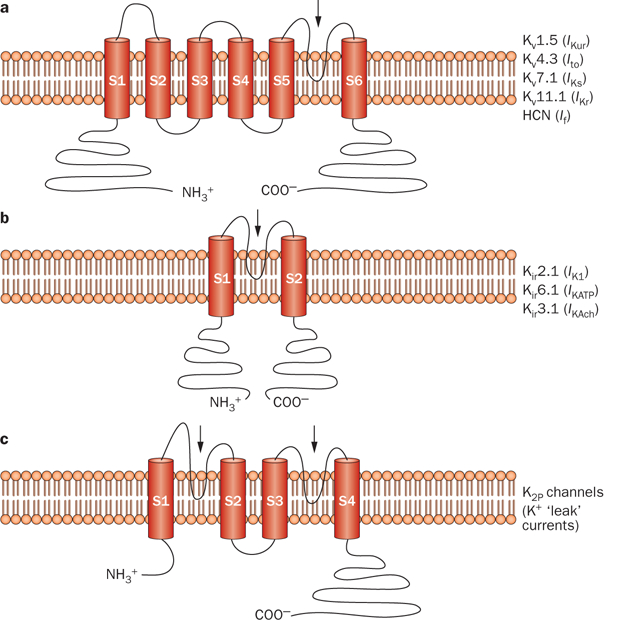
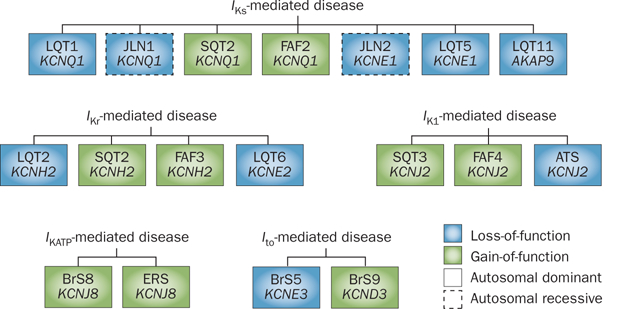
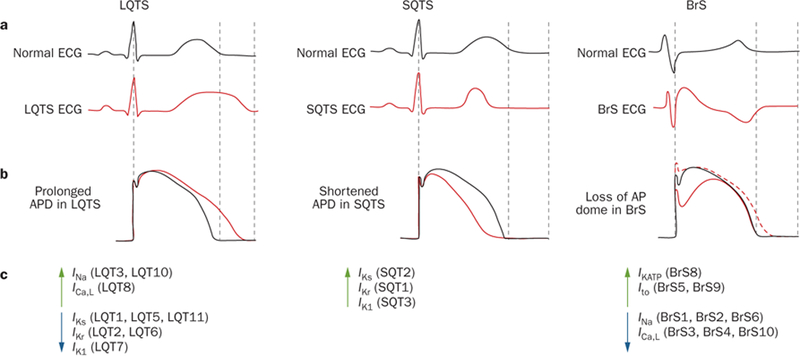
The coordinated generation and propagation of action potentials within cardiomyocytes creates the intrinsic electrical stimuli that are responsible for maintaining the electromechanical pump function of the human heart. The synchronous opening and closing of cardiac Na(+), Ca(2+), and K(+) channels corresponds with the activation and inactivation of inward depolarizing (Na(+) and Ca(2+)) and outward repolarizing (K(+)) currents that underlie the various phases of the cardiac action potential (resting, depolarization, plateau, and repolarization). Inherited mutations in pore-forming α subunits and accessory β subunits of cardiac K(+) channels can perturb the atrial and ventricular action potential and cause various cardiac arrhythmia syndromes, including long QT syndrome, short QT syndrome, Brugada syndrome, and familial atrial fibrillation. In this Review, we summarize the current understanding of the molecular and cellular mechanisms that underlie K(+)-channel-mediated arrhythmia syndromes. We also describe translational advances that have led to the emerging role of genetic testing and genotype-specific therapy in the diagnosis and clinical management of individuals who harbor pathogenic mutations in genes that encode α or β subunits of cardiac K(+) channels.
Conflict of interest statement
Competing interests
M. J. Ackerman declares associations with the following companies: Biotronik, Boston Scientific, Medtronic, St. Jude Medical, and Transgenomic. See the article online for full details of the relationships. J. R. Giudicessi declares no competing interests.
Figures
References
-
- Nerbonne JM & Kass RS Molecular physiology of cardiac repolarization. Physiol. Rev 85, 1205–1253 (2005). - PubMed
-
- Wang Q et al. Positional cloning of a novel potassium channel gene: KVLQT1 mutations cause cardiac arrhythmias. Nat. Genet 12, 17–23 (1996). - PubMed
-
- Curran ME et al. A molecular basis for cardiac arrhythmia: HERG mutations cause long QT syndrome. Cell 80, 795–803 (1995). - PubMed
-
- Plaster NM et al. Mutations in Kir2.1 cause the developmental and episodic electrical phenotypes of Andersen’s syndrome. Cell 105, 511–519 (2001). - PubMed
-
- Hedley PL et al. The genetic basis of Brugada syndrome: a mutation update. Hum. Mutat 30, 1256–1266 (2009). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
