

Review
doi: 10.1097/PPO.0b013e3182431a73.
Immunotherapy for the treatment of glioblastoma
Affiliations
- PMID: 22290259
- PMCID: PMC3269657
- DOI: 10.1097/PPO.0b013e3182431a73
Item in Clipboard
Review
Immunotherapy for the treatment of glioblastoma
Cancer J.
2012 Jan-Feb.
Abstract
Glioblastoma, the most aggressive primary brain tumor, thrives in a microenvironment of relative immunosuppression within the relatively immune-privileged central nervous system. Despite treatments with surgery, radiation therapy, and chemotherapy, prognosis remains poor. The recent success of immunotherapy in the treatment of other cancers has renewed interest in vaccine therapy for the treatment of gliomas. In this article, we outline various immunotherapeutic strategies, review recent clinical trials data, and discuss the future of vaccine therapy for glioblastoma.
Figures
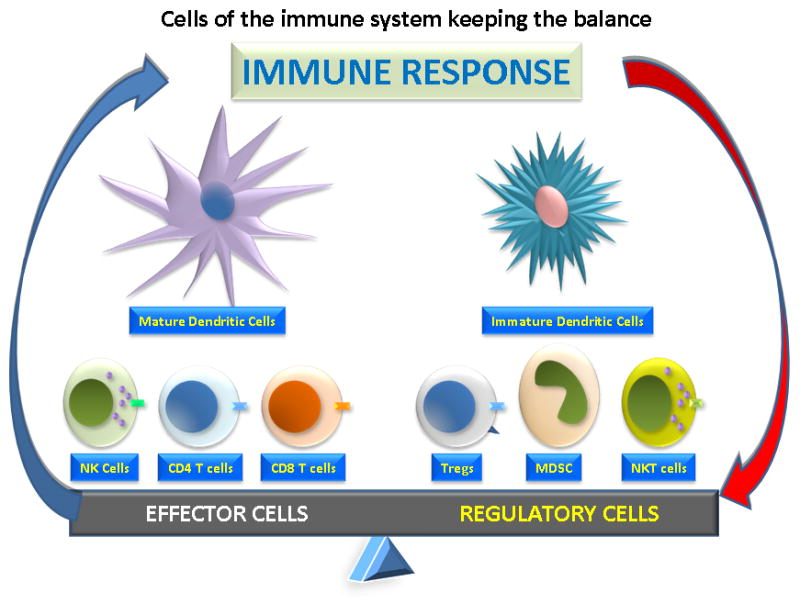
Cells of the immune system include effector cells and regulatory cells. Among the effector cells are CD4+ helper T cells, CD8+ cytotoxic T lymphocytes (CTL), natural killer cells (NK) and dendritic cells (DC), which are the antigen presenting cells. The regulatory cells include regulatory T cells (Treg), which express CD4, CD25 and CTLA4, and myeloid-derived suppressor cells (MDSC).
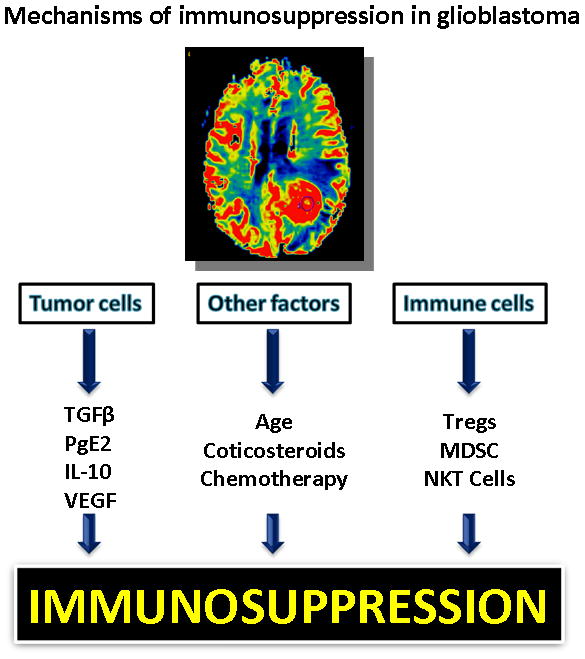
Factors contributing to immunosuppression in glioblastoma include tumor factors, exogenous factors, and immune factors. The glioma cells secrete immunosuppressive cytokines, such as TGFβ, prostaglandin E2, IL-10, and VEGF. Age, exogenous steroids, and chemotherapy all contribute to exogenous immune suppression; while regulatory immune cells such as regulatory T cells (Treg) and myeloid derived suppressor cells (MDSC), also dampen the immune response.
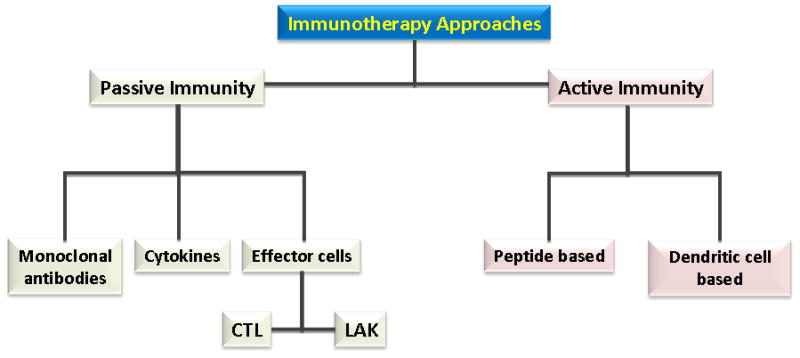
Approaches to immunotherapy can be divided into passive immunity and active immunity. Passive immunotherapy approaches include direct administration of monoclonal antibodies or cytokines or adoptive immunity with cytotoxic T lymphocytes (CTL) or lymphocyte activated killer (LAK) cells. Active immunity includes peptide based immunotherapy and dendritic cell therapy.
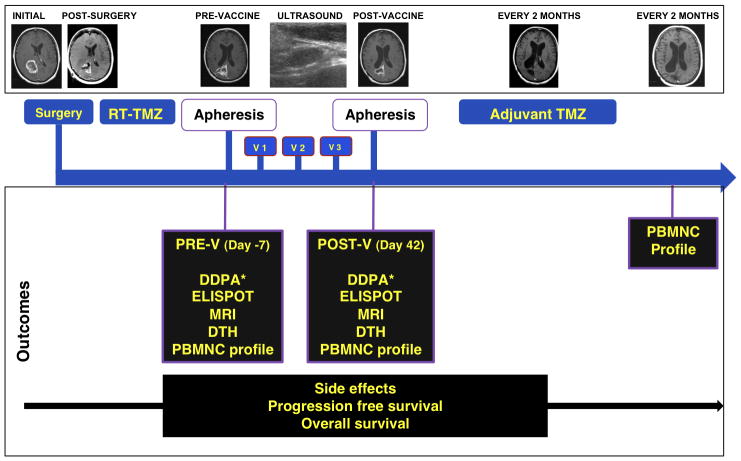
Four weeks after complete combined RT-TMZ, patients had a prevaccination (V) aphesis, DTH panel placement, and MRI. One week later, the first vaccination (V1) was administered, and 2 additional vaccinations were given 2 weeks apart. Two weeks after the third vaccine patients had a post-V apheresis, DTH panel placement, and MRI, followed by 12 cycles of adjuvant TMZ. DDPA indicates dye dilution proliferation assay; DTH, delayed-type hypersensitivity reaction; ELISPOT, enzyme-liked immunosorbent spot assay; PBMNC, peripheral blood mononuclear cells; POST-V, postvaccination; PRE-V, prevaccination; RT, radiation therapy; TMZ, temozolomide; v, vaccination. Printed with permission from Fadul et al, 2011 .
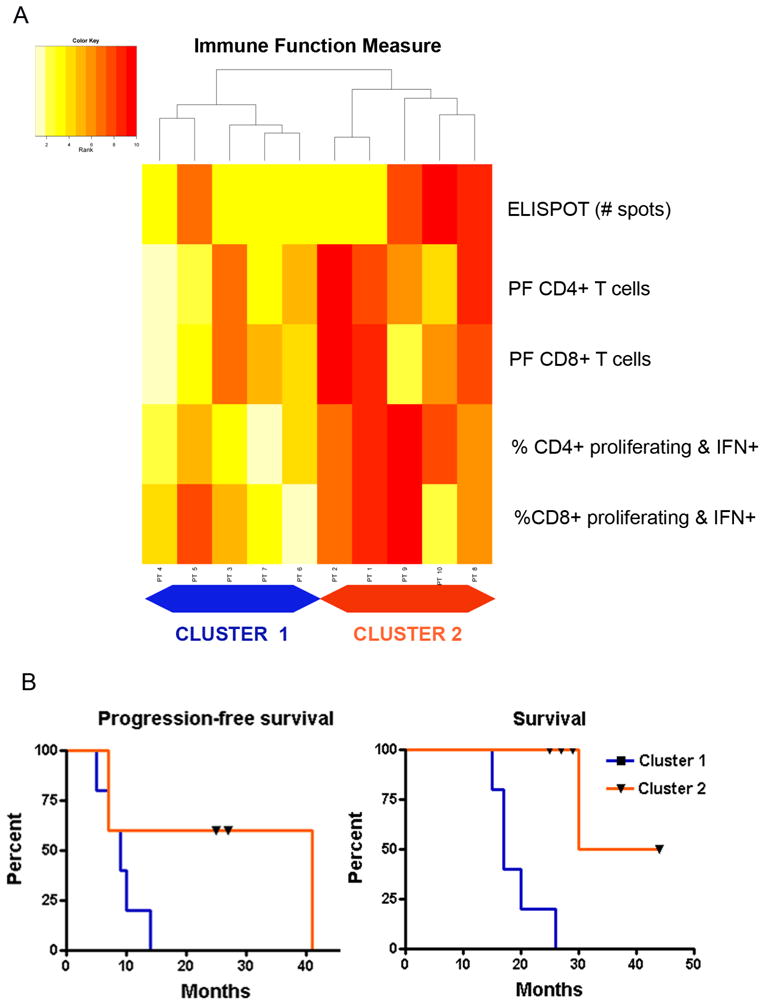
(5A) Heatmap of hierarchical clustering analysis of the postvaccination immune responses. Five patients with generally low ranks in immune function (pale yellow colors) formed cluster 1 on the left. Five other patients with higher ranks in immune function measures (dark red colors) formed cluster 2 on the right. (5B) Kaplan-Meier curve of overall survival for the 2 clusters. The overall survival was significantly different between cluster 1 (median = 17 mo) and cluster 2 (median = not achieved) (P = 0.002). ELISPOT indicates enzyme-linked immunosorbent spot assay; IFN, interferon; PF, precursor frequency. Printed with permission from Fadul et al, 2011 .
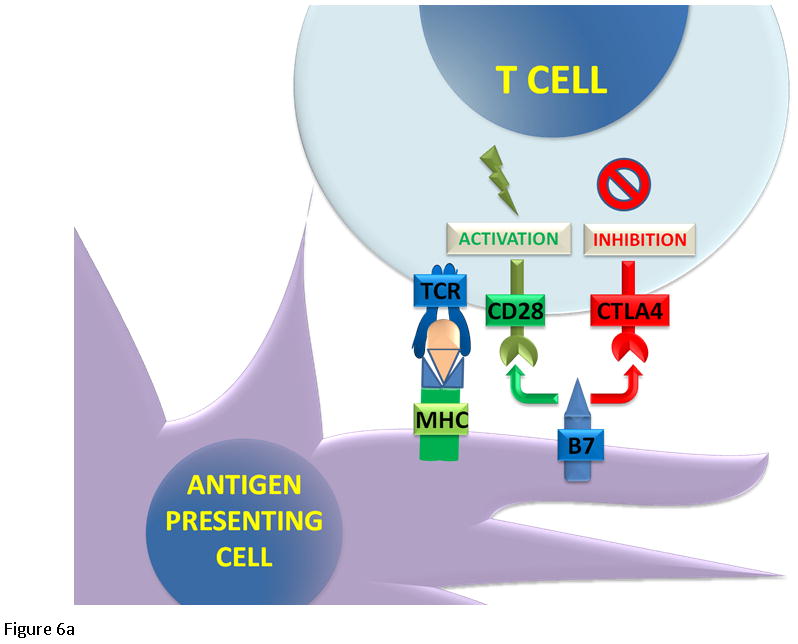
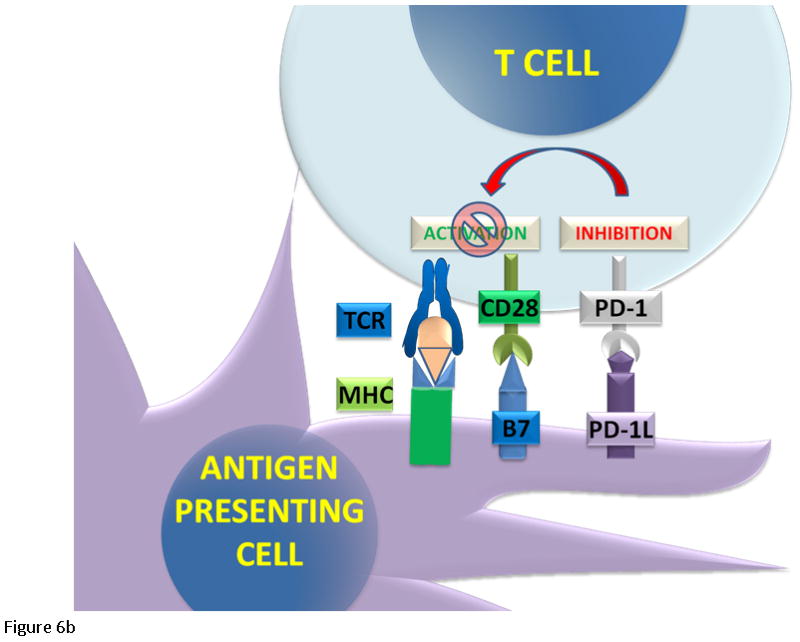
T cell regulation. (6A) The cytotoxic T cells express CD8 receptor that binds to the MHC receptor on the APC, along with a second signal mediated by CD28 binding to its ligand B7. The binding of the T cell receptor and CD28 lead to activation and cell mediated killing. Activated T cells upregulate CTLA4 and PD-1 proteins. CTLA4 competes with CD28 to bind B7. (6B) When PD-1 binds to its ligand PD-L1, it inhibits T cell activation.
T cell regulation. (6A) The cytotoxic T cells express CD8 receptor that binds to the MHC receptor on the APC, along with a second signal mediated by CD28 binding to its ligand B7. The binding of the T cell receptor and CD28 lead to activation and cell mediated killing. Activated T cells upregulate CTLA4 and PD-1 proteins. CTLA4 competes with CD28 to bind B7. (6B) When PD-1 binds to its ligand PD-L1, it inhibits T cell activation.
References
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352:987–96. - PubMed
-
- Dillman RO. Cancer immunotherapy. Cancer Biother Radiopharm. 2011;26:1–64. - PubMed
-
- Abbas . Diseases of Immunity. In: Fausto KA, editor. Robbins and Cotran Pathologic Basis of Disease. 7. Philadelphia: Elsevier Saunders; 2005. pp. 193–267.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
