

Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study
- PMID: 22291074
- PMCID: PMC3295548
- DOI: 10.1200/JCO.2011.38.8645
Recurrence and survival after random assignment to laparoscopy versus laparotomy for comprehensive surgical staging of uterine cancer: Gynecologic Oncology Group LAP2 Study
Erratum in
- J Clin Oncol. 2012 May 1;30(13):1570
Abstract
Purpose: The primary objective was to establish noninferiority of laparoscopy compared with laparotomy for recurrence after surgical staging of uterine cancer.
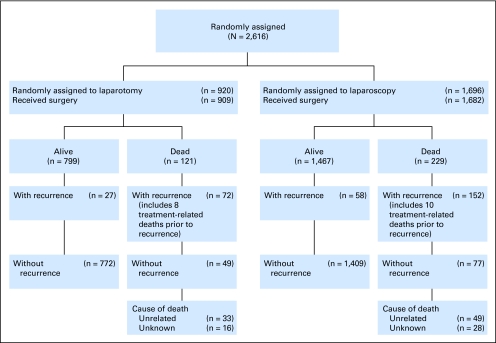
Patients and methods: Patients with clinical stages I to IIA disease were randomly allocated (two to one) to laparoscopy (n = 1,696) versus laparotomy (n = 920) for hysterectomy, salpingo-oophorectomy, pelvic cytology, and pelvic and para-aortic lymphadenectomy. The primary study end point was noninferiority of recurrence-free interval defined as no more than a 40% increase in the risk of recurrence with laparoscopy compared with laparotomy.
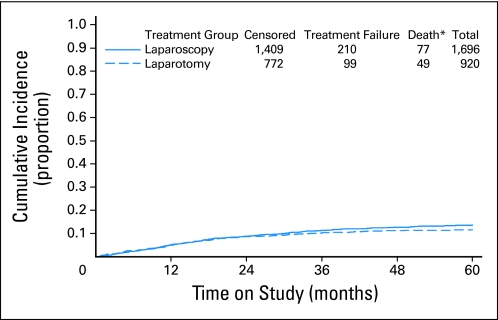
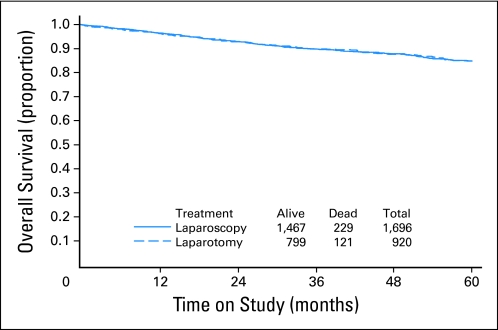
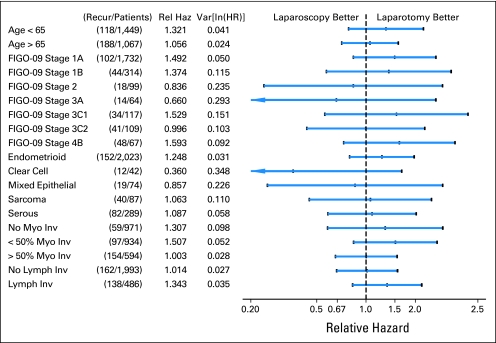
Results: With a median follow-up time of 59 months for 2,181 patients still alive, there were 309 recurrences (210 laparoscopy; 99 laparotomy) and 350 deaths (229 laparoscopy; 121 laparotomy). The estimated hazard ratio for laparoscopy relative to laparotomy was 1.14 (90% lower bound, 0.92; 95% upper bound, 1.46), falling short of the protocol-specified definition of noninferiority. However, the actual recurrence rates were substantially lower than anticipated, resulting in an estimated 3-year recurrence rate of 11.4% with laparoscopy and 10.2% with laparotomy, or a difference of 1.14% (90% lower bound, -1.28; 95% upper bound, 4.0). The estimated 5-year overall survival was almost identical in both arms at 89.8%.
Conclusion: This study previously reported that laparoscopic surgical management of uterine cancer is superior for short-term safety and length-of-stay end points. The potential for increased risk of cancer recurrence with laparoscopy versus laparotomy was quantified and found to be small, providing accurate information for decision making for women with uterine cancer.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures
Comment in
-
Minimally invasive surgery for endometrial cancer: the horse is already out of the barn.J Clin Oncol. 2012 Mar 1;30(7):681-2. doi: 10.1200/JCO.2011.40.5506. Epub 2012 Jan 30. J Clin Oncol. 2012. PMID: 22291090 No abstract available.
References
-
- Jemal A, Siegel R, Xu J, et al. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Mutch DG. The New FIGO staging system for cancers of the vulva, cervix, endometrium, and sarcomas. Gynecol Oncol. 2009;115:325–328.
-
- Creasman WT, Morrow CP, Bundy BN, et al. Surgical pathologic spread patterns of endometrial cancer. Cancer. 1987;60:2035–2041. - PubMed
-
- Morrow CP, Bundy BN, Kurman FJ, et al. Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: A Gynecologic Oncology Group Study. Gynecol Oncol. 1991;40:55–65. - PubMed
-
- Bristow RE, Zerbe MJ, Rosenshein NB, et al. Stage IVB endometrial carcinoma: The role of cytoreductive surgery and determinants of survival. Gynecol Oncol. 2000;78:85–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
