

ARID5B genetic polymorphisms contribute to racial disparities in the incidence and treatment outcome of childhood acute lymphoblastic leukemia
- PMID: 22291082
- PMCID: PMC3295551
- DOI: 10.1200/JCO.2011.38.0345
ARID5B genetic polymorphisms contribute to racial disparities in the incidence and treatment outcome of childhood acute lymphoblastic leukemia
Abstract
Purpose: Recent genome-wide screens have identified genetic variations in ARID5B associated with susceptibility to childhood acute lymphoblastic leukemia (ALL). We sought to determine the contribution of ARID5B single nucleotide polymorphisms (SNPs) to racial disparities in ALL susceptibility and treatment outcome.
Patients and methods: We compared the association between ARID5B SNP genotype and ALL susceptibility in whites (> 95% European genetic ancestry; 978 cases and 1,046 controls) versus in Hispanics (> 10% Native American ancestry; 330 cases and 541 controls). We determined the relationships between ARID5B SNP genotype and ALL relapse risk in 1,605 children treated on the Children's Oncology Group (COG) P9904/9905 clinical trials.
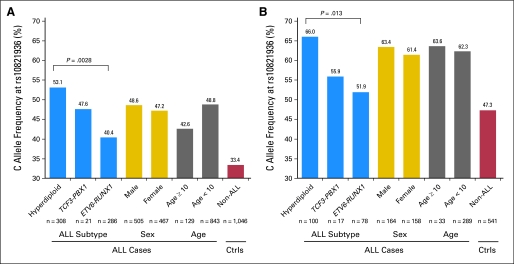
Results: Among 49 ARID5B SNPs interrogated, 10 were significantly associated with ALL susceptibility in both whites and Hispanics (P < .05), with risk alleles consistently more frequent in Hispanics than in whites. rs10821936 exhibited the most significant association in both races (P = 8.4 × 10(-20) in whites; P = 1 × 10(-6) in Hispanics), and genotype at this SNP was highly correlated with local Native American genetic ancestry (P = 1.8 × 10(-8)). Multivariate analyses in Hispanics identified an additional SNP associated with ALL susceptibility independent of rs10821936. Eight ARID5B SNPs were associated with both ALL susceptibility and relapse hazard; the alleles related to higher ALL incidence were always linked to poorer treatment outcome and were more frequent in Hispanics.
Conclusion: ARID5B polymorphisms are important determinants of childhood ALL susceptibility and treatment outcome, and they contribute to racial disparities in this disease.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest and author contributions are found at the end of this article.
Figures


References
-
- Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006;354:166–178. - PubMed
-
- McNeil DE, Coté TR, Clegg L, et al. SEER update of incidence and trends in pediatric malignancies: Acute lymphoblastic leukemia. Med Pediatr Oncol. 2002;39:554–557. discussion 552-553. - PubMed
-
- Linabery AM, Ross JA. Trends in childhood cancer incidence in the U.S. (1992-2004) Cancer. 2008;112:416–432. - PubMed
-
- Horner MJ, Ries LAG, Krapcho M, et al. Bethesda, MD: National Cancer Institute; 2009. SEER Cancer Statistics Review, 1975-2006.
Publication types
MeSH terms
Substances
Grants and funding
- R21 CA158568/CA/NCI NIH HHS/United States
- UL1 TR000064/TR/NCATS NIH HHS/United States
- U01GM61393/GM/NIGMS NIH HHS/United States
- CA114762/CA/NCI NIH HHS/United States
- CA114766/CA/NCI NIH HHS/United States
- R01 CA078224/CA/NCI NIH HHS/United States
- P30 CA021765/CA/NCI NIH HHS/United States
- U01 CA157937/CA/NCI NIH HHS/United States
- U10 CA098543/CA/NCI NIH HHS/United States
- RC4CA156449/CA/NCI NIH HHS/United States
- CA021765-33/CA/NCI NIH HHS/United States
- R01 HL088133/HL/NHLBI NIH HHS/United States
- HL088133/HL/NHLBI NIH HHS/United States
- U01 GM092666/GM/NIGMS NIH HHS/United States
- CA98543/CA/NCI NIH HHS/United States
- U01 GM061393/GM/NIGMS NIH HHS/United States
- U10CA98413/CA/NCI NIH HHS/United States
- U01 CA114762/CA/NCI NIH HHS/United States
- U10 CA098413/CA/NCI NIH HHS/United States
- U24 CA114766/CA/NCI NIH HHS/United States
- CA093552/CA/NCI NIH HHS/United States
- RC4 CA156449/CA/NCI NIH HHS/United States
- CA21765/CA/NCI NIH HHS/United States
- CA78224/CA/NCI NIH HHS/United States
- R21CA158568/CA/NCI NIH HHS/United States
- U01GM92666/GM/NIGMS NIH HHS/United States
- R01 CA093552/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
