

Inhaled treprostinil: a therapeutic review
- PMID: 22291467
- PMCID: PMC3267519
- DOI: 10.2147/DDDT.S19281
Inhaled treprostinil: a therapeutic review
Abstract
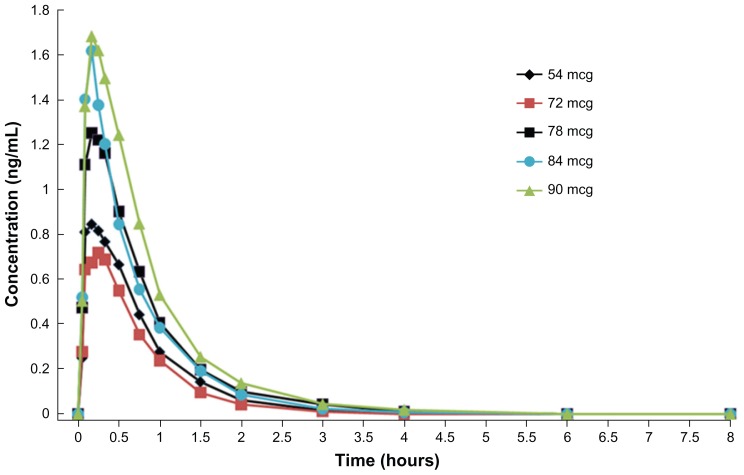
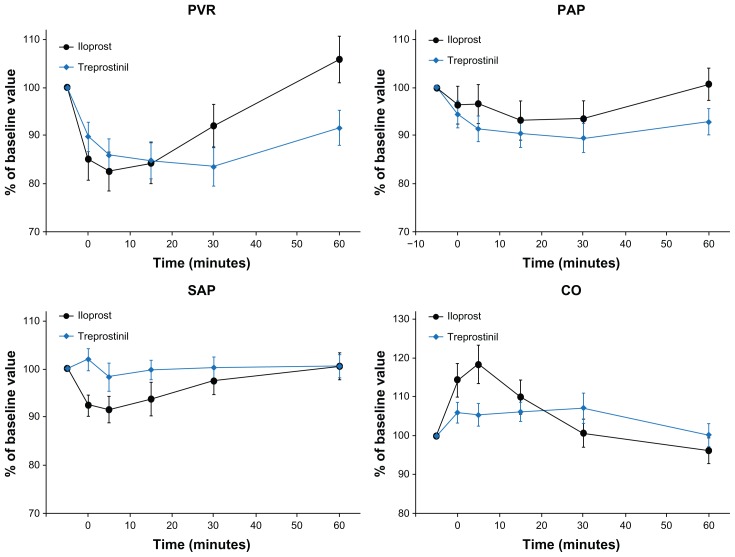
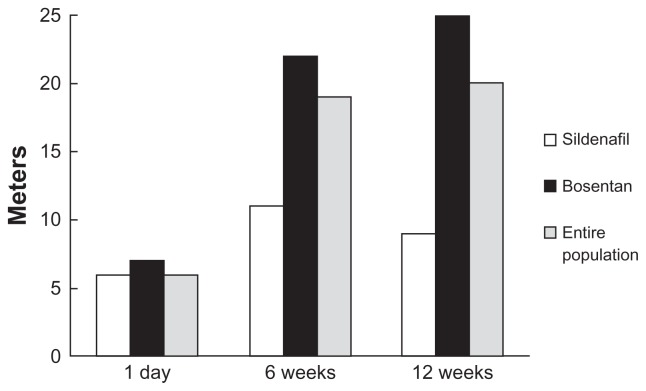
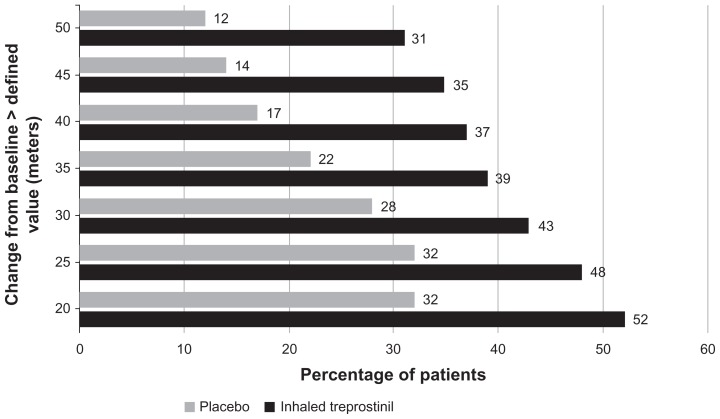
Pulmonary arterial hypertension (PAH) is a life-threatening disease which, if untreated, leads to right ventricular failure and often death. Several effective therapies are now available for PAH, including endothelin receptor antagonists, phosphodiesterase-5 inhibitors, and prostacyclin analogs. The prostacyclin analog treprostinil has proven efficacious when delivered by subcutaneous or intravenous infusion, and most recently by inhalation. Inhaled treprostinil has been shown to be 64%-72% bioavailable in healthy volunteers. Pilot clinical studies have elucidated the acute hemodynamic effects and relative pulmonary selectivity of this agent, as well as established target dosing in PAH and nonoperable chronic thromboembolic PAH. Likewise, chronically administered inhaled treprostinil resulted in clinical and hemodynamic improvement. Both pilot studies confirmed a satisfactory safety profile in patients with PAH. The pivotal Phase III trial, TRIUMPH-I, demonstrated the efficacy and safety of inhaled treprostinil (target dose of 54 μg four times daily) in PAH patients added to background therapies of bosentan or sildenafil, as assessed by improvements in the primary endpoint, peak six-minute walk distance (median placebo-corrected treatment effect of 20 m), as well as select secondary endpoints. Inhaled treprostinil is approved by the US Food and Drug Administration for patients with World Health Organization Group I PAH to improve exercise ability. Studies establishing effectiveness included predominately patients with New York Heart Association functional class III symptoms and etiologies of idiopathic or heritable PAH (56%) or PAH associated with connective tissue diseases (33%).
Keywords: inhaled; nebulizer; prostacyclin; pulmonary arterial hypertension; treprostinil.
Figures

References
-
- D’Alonzo GE, Barst RJ, Ayres SM, et al. Survival in patients with primary pulmonary hypertension. Results from a national prospective registry. Ann Intern Med. 1991;115:343–349. - PubMed
-
- Barst RJ, Rubin LJ, Long WA, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. The Primary Pulmonary Hypertension Study Group. N Engl J Med. 1996;334:296–302. - PubMed
-
- Simonneau G, Barst RJ, Galie N, et al. Treprostinil Study Group. Continuous subcutaneous infusion of treprostinil, a prostacyclin analog, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. 2002;165:800–804. - PubMed
-
- Olschewski H, Simonneau G, Galie N, et al. Aerosolized Iloprost Randomized Study Group. Inhaled iloprost for severe pulmonary hypertension. N Engl J Med. 2002;347:322–329. - PubMed
-
- Channick RN, Simonneau G, Sitbon O, et al. Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomized placebo-controlled study. Lancet. 2001;358:1119–1123. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
