

Tramiprosate in mild-to-moderate Alzheimer's disease - a randomized, double-blind, placebo-controlled, multi-centre study (the Alphase Study)
- PMID: 22291741
- PMCID: PMC3258678
- DOI: 10.5114/aoms.2011.20612
Tramiprosate in mild-to-moderate Alzheimer's disease - a randomized, double-blind, placebo-controlled, multi-centre study (the Alphase Study)
Abstract
Introduction: The aim of the study was to assess the clinical efficacy, safety, and disease-modification effects of tramiprosate (homotaurine, ALZHEMED(TM)) in mild-to-moderate Alzheimer's disease (AD).
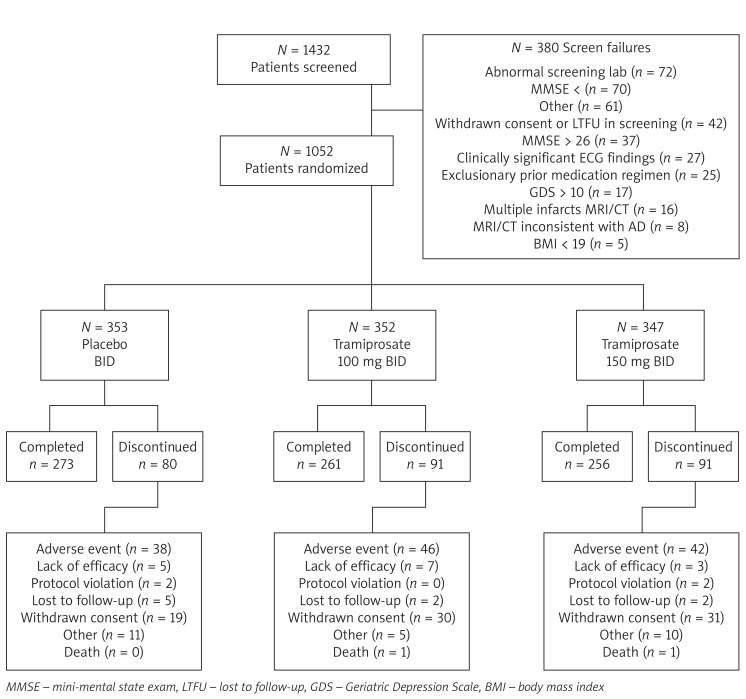
Material and methods: Double-blind, placebo-controlled, randomized trial in 67 clinical centres across North America. Patients aged ≥ 50 years, with mild-to-moderate AD (Mini-Mental State Examination score between 16 and 26) and on stable doses of cholinesterase inhibitors, alone or with memantine.
Intervention: 78-week treatment with placebo, tramiprosate 100 mg or tramiprosate 150 mg BID.
Measurements: Alzheimer Disease Assessment Scale - cognitive subscale (ADAS-cog) and Clinical Dementia Rating - Sum of Boxes (CDR-SB) assessments were performed at baseline and every 13 weeks. Baseline and 78-week magnetic resonance imaging (MRI) hippocampus volume (HV) measurements were conducted in a subgroup of patients.
Results: A total of 1,052 patients were enrolled and 790 (75.1%) completed the 78-week trial. Patient discontinuation and reasons for withdrawal were similar across groups. Planned analyses did not reveal statistically significant between-group differences. Lack of adequate statistical validity of the planned analysis models led to the development of revised predictive models. These adjusted models showed a trend toward a treatment effect for ADAS-cog (P = 0.098) and indicated significantly less HV loss for tramiprosate 100 mg (P = 0.035) and 150 mg (P = 0.009) compared to placebo. The incidence of adverse events was similar across treatment groups.
Conclusions: The primary planned analyses did not show a significant treatment effect, but were confounded by unexplained variance. Post-hoc analyses showed a significant treatment-related reduction in HV loss. However, there was only a trend towards slowing of decline on the ADAS-cog and no slowing of decline on the CDR-SB. These results must be interpreted in consideration of the limitations of clinical and disease-modification outcome measures and their relationship, the heterogeneity of the disease and the impact of confounding demographic and clinical variables.
Keywords: Alzheimer’s disease; amyloid; disease-modification; tramiprosate; volumetric MRI.
References
-
- Canevari L, Abramov A, Duchen MR. Toxicity of amyloid B peptide tales of calcium, mitochondria and oxidative stress. Neurochem Res. 2004;29:637–50. - PubMed
-
- Citron M. Strategies for disease modification in Alzheimer’s disease. Nat Rev Neurosci. 2004;5:677–85. - PubMed
-
- Gervais F, Paquette J, Morissette C. Targeting soluble Abeta peptide with Tramiprosate for the treatment of brain amyloidosis. Neurobiol Aging. 2007;28:537–47. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources