

Gene-expression signature predicts postoperative recurrence in stage I non-small cell lung cancer patients
- PMID: 22292069
- PMCID: PMC3264655
- DOI: 10.1371/journal.pone.0030880
Gene-expression signature predicts postoperative recurrence in stage I non-small cell lung cancer patients
Abstract
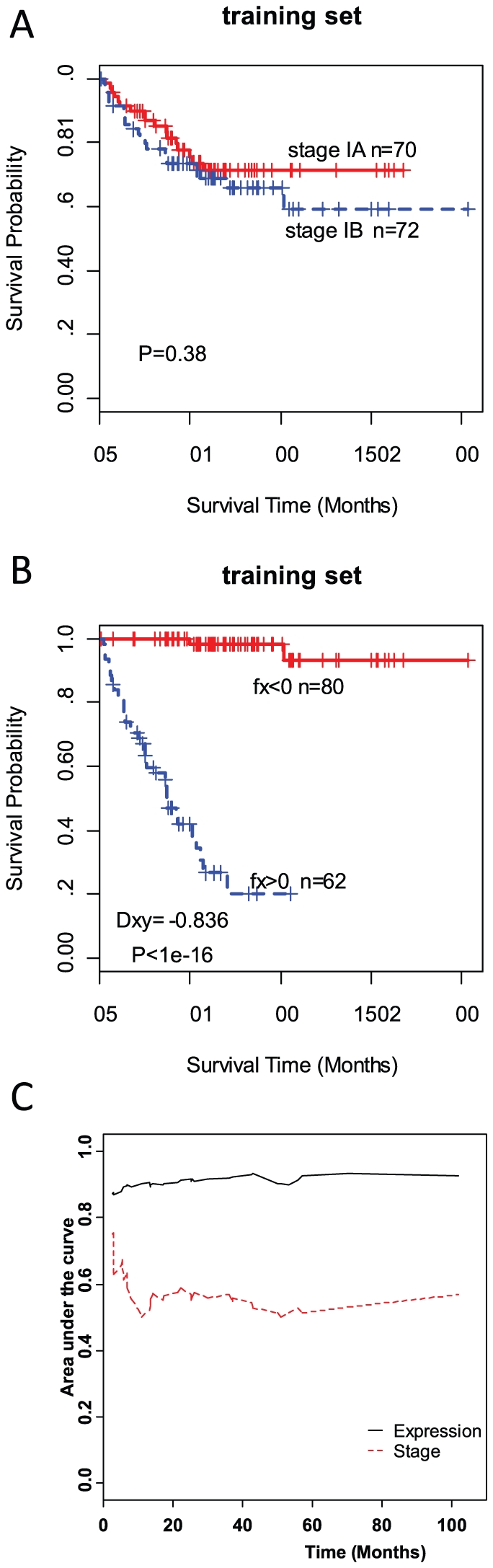
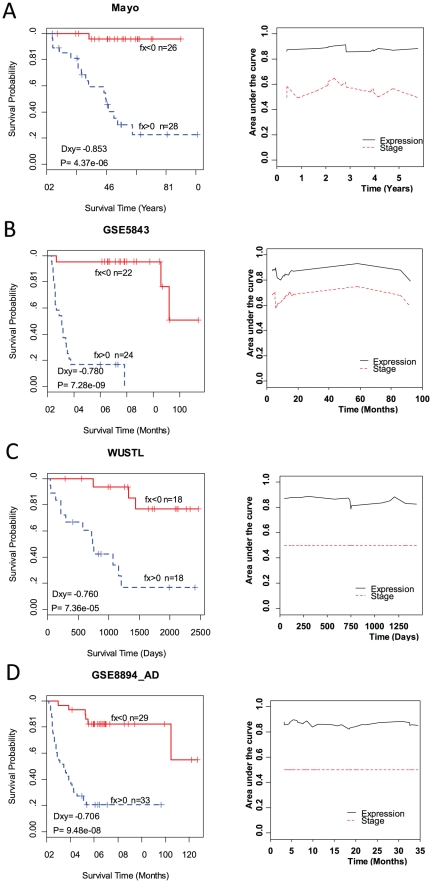
About 30% stage I non-small cell lung cancer (NSCLC) patients undergoing resection will recur. Robust prognostic markers are required to better manage therapy options. The purpose of this study is to develop and validate a novel gene-expression signature that can predict tumor recurrence of stage I NSCLC patients. Cox proportional hazards regression analysis was performed to identify recurrence-related genes and a partial Cox regression model was used to generate a gene signature of recurrence in the training dataset -142 stage I lung adenocarcinomas without adjunctive therapy from the Director's Challenge Consortium. Four independent validation datasets, including GSE5843, GSE8894, and two other datasets provided by Mayo Clinic and Washington University, were used to assess the prediction accuracy by calculating the correlation between risk score estimated from gene expression and real recurrence-free survival time and AUC of time-dependent ROC analysis. Pathway-based survival analyses were also performed. 104 probesets correlated with recurrence in the training dataset. They are enriched in cell adhesion, apoptosis and regulation of cell proliferation. A 51-gene expression signature was identified to distinguish patients likely to develop tumor recurrence (Dxy = -0.83, P<1e-16) and this signature was validated in four independent datasets with AUC >85%. Multiple pathways including leukocyte transendothelial migration and cell adhesion were highly correlated with recurrence-free survival. The gene signature is highly predictive of recurrence in stage I NSCLC patients, which has important prognostic and therapeutic implications for the future management of these patients.
Conflict of interest statement
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. - PubMed
-
- Flehinger BJ, Kimmel M, Melamed MR. The effect of surgical treatment on survival from early lung cancer. Implications for screening. Chest. 1992;101:1013–1018. - PubMed
-
- Strauss GM, Kwiatkowski DJ, Harpole DH, Lynch TJ, Skarin AT, et al. Molecular and pathologic markers in stage I non-small-cell carcinoma of the lung. J Clin Oncol. 1995;13:1265–1279. - PubMed
-
- Douillard JY, Rosell R, De Lena M, Carpagnano F, Ramlau R, et al. Adjuvant vinorelbine plus cisplatin versus observation in patients with completely resected stage IB-IIIA non-small-cell lung cancer (Adjuvant Navelbine International Trialist Association [ANITA]): a randomised controlled trial. Lancet Oncol. 2006;7:719–727. - PubMed
-
- Le Chevalier T, Lynch T. Adjuvant treatment of lung cancer: current status and potential applications of new regimens. Lung Cancer. 2004;46(Suppl 2):S33–39. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
