

Minimally invasive intrathoracic anastomosis after Ivor Lewis esophagectomy for cancer: a review of transoral or transthoracic use of staplers
- PMID: 22294057
- PMCID: PMC3372777
- DOI: 10.1007/s00464-012-2149-z
Minimally invasive intrathoracic anastomosis after Ivor Lewis esophagectomy for cancer: a review of transoral or transthoracic use of staplers
Abstract
Background: Minimally invasive Ivor Lewis esophagectomy is one of the approaches used worldwide for treating esophageal cancer. Optimization of this approach and especially identifying the ideal intrathoracic anastomosis technique is needed. To date, different types of anastomosis have been described. A literature search on the current techniques and approaches for intrathoracic anastomosis was held. The studies were evaluated on leakage and stenosis rate of the anastomosis.
Methods: The PubMed electronic database was used for comprehensive literature search by two independent reviewers.
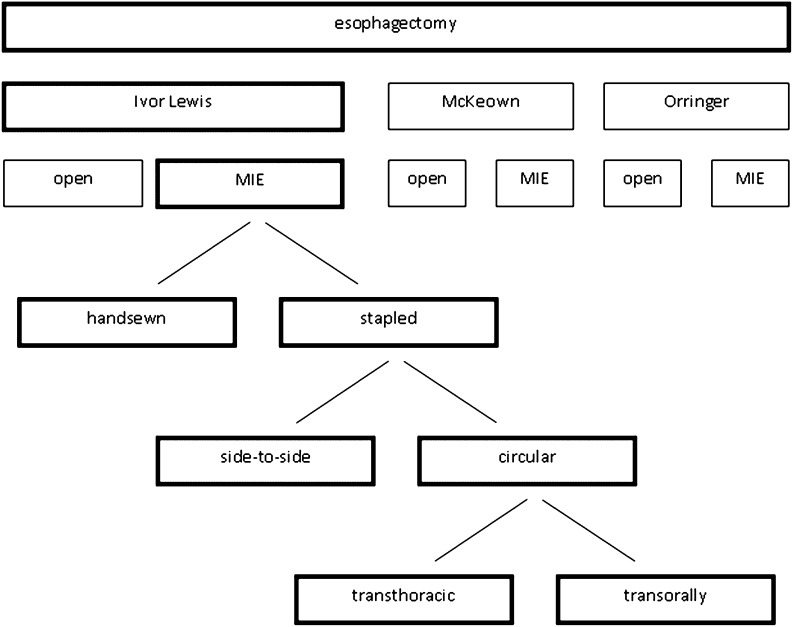
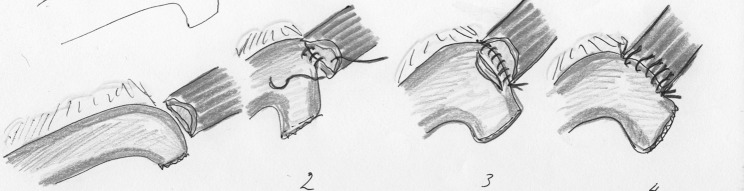
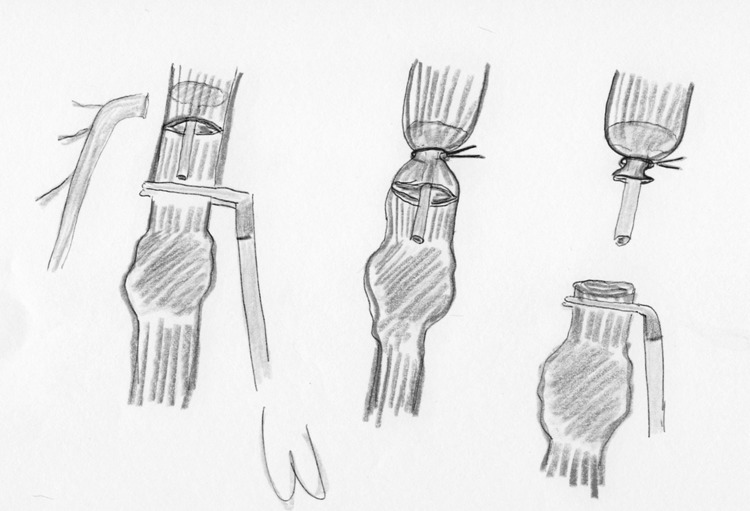
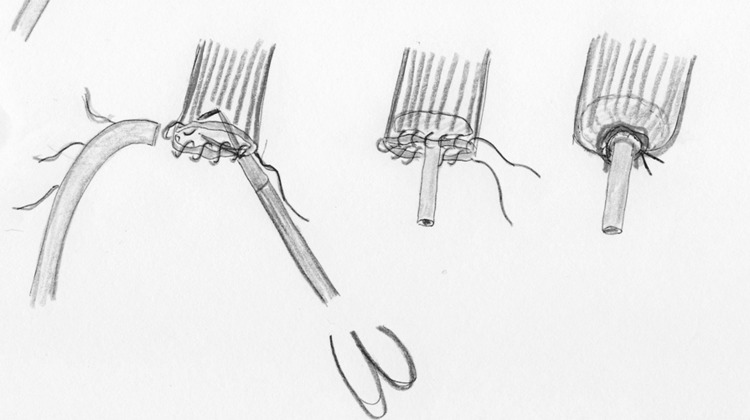
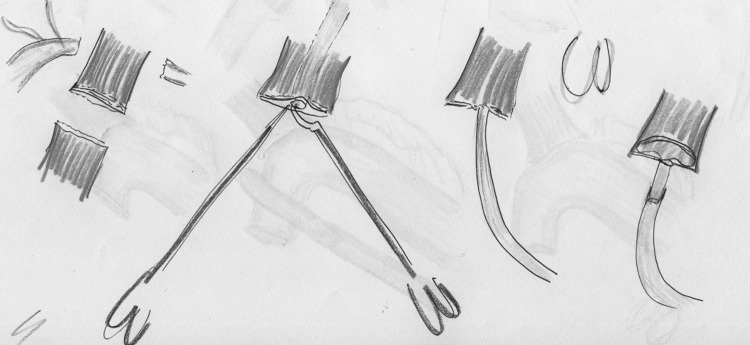
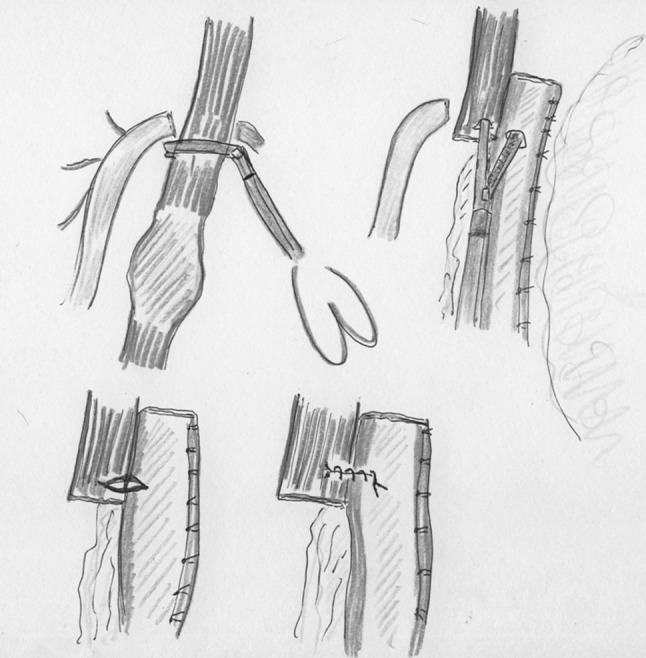
Results: Twelve studies were included in this review. The most frequent applied technique was the stapled anastomosis. Stapled anastomoses can be divided into a transthoracic or a transoral introduction. This stapled approach can be performed with a circular or linear stapler. The reported anastomotic leakage rate ranges from 0 to 10%. The reported anastomotic stenosis rate ranges from 0 to 27.5%.
Conclusions: This review has found no important differences between the two most frequently used stapled anastomoses: the transoral introduction of the anvil and the transthoracic. Clinical trials are needed to compare different methods to improve the quality of the intrathoracic anastomosis after esophagectomy.
Figures
References
-
- Orringer MB, Sloan H. Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg. 1978;76:643–654. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
