

Effect of n-3 long chain polyunsaturated fatty acid supplementation in pregnancy on infants' allergies in first year of life: randomised controlled trial
- PMID: 22294737
- PMCID: PMC3269207
- DOI: 10.1136/bmj.e184
Effect of n-3 long chain polyunsaturated fatty acid supplementation in pregnancy on infants' allergies in first year of life: randomised controlled trial
Abstract
Objective: To determine whether dietary n-3 long chain polyunsaturated fatty acid (LCPUFA) supplementation of pregnant women with a fetus at high risk of allergic disease reduces immunoglobulin E associated eczema or food allergy at 1 year of age.
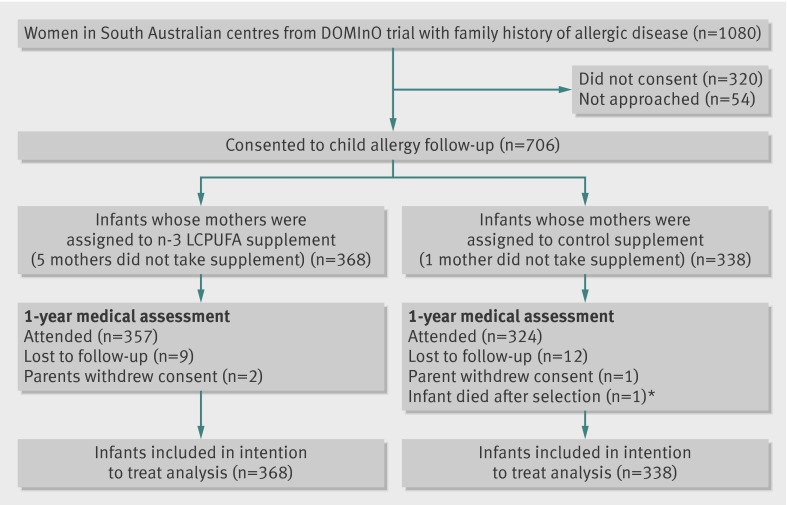
Design: Follow-up of infants at high hereditary risk of allergic disease in the Docosahexaenoic Acid to Optimise Mother Infant Outcome (DOMInO) randomised controlled trial.
Setting: Adelaide, South Australia.
Participants: 706 infants at high hereditary risk of developing allergic disease whose mothers were participating in the DOMInO trial.
Interventions: The intervention group (n=368) was randomly allocated to receive fish oil capsules (providing 900 mg of n-3 LCPUFA daily) from 21 weeks' gestation until birth; the control group (n=338) received matched vegetable oil capsules without n-3 LCPUFA.
Main outcome measure: Immunoglobulin E associated allergic disease (eczema or food allergy with sensitisation) at 1 year of age.
Results: No differences were seen in the overall percentage of infants with immunoglobulin E associated allergic disease between the n-3 LCPUFA and control groups (32/368 (9%) v 43/338 (13%); unadjusted relative risk 0.68, 95% confidence interval 0.43 to 1.05, P=0.08; adjusted relative risk 0.70, 0.45 to 1.09, P=0.12), although the percentage of infants diagnosed as having atopic eczema (that is, eczema with associated sensitisation) was lower in the n-3 LCPUFA group (26/368 (7%) v 39/338 (12%); unadjusted relative risk 0.61, 0.38 to 0.98, P=0.04; adjusted relative risk 0.64, 0.40 to 1.02, P=0.06). Fewer infants were sensitised to egg in the n-3 LCPUFA group (34/368 (9%) v 52/338 (15%); unadjusted relative risk 0.61, 0.40 to 0.91, P=0.02; adjusted relative risk 0.62, 0.41 to 0.93, P=0.02), but no difference between groups in immunoglobulin E associated food allergy was seen.
Conclusion: n-3 LCPUFA supplementation in pregnancy did not reduce the overall incidence of immunoglobulin E associated allergies in the first year of life, although atopic eczema and egg sensitisation were lower. Longer term follow-up is needed to determine if supplementation has an effect on respiratory allergic diseases and aeroallergen sensitisation in childhood.
Trial registration: Australian New Zealand Clinical Trials Registry ACTRN12610000735055 (DOMInO trial: ACTRN12605000569606).
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Asher MI, Montefort S, Bjorksten B, Lai CK, Strachan DP, Weiland SK, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet 2006;368:733-43. - PubMed
-
- International Study of Asthma and Allergies in Childhood Steering Committee (ISSAC). Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998;351:1225-32. - PubMed
-
- Robertson CF, Roberts MF, Kappers JH. Asthma prevalence in Melbourne schoolchildren: have we reached the peak? Med J Aust 2004;180:273-6. - PubMed
-
- Gupta R, Sheikh A, Strachan DP, Anderson HR. Burden of allergic disease in the UK: secondary analyses of national databases. Clin Exp Allergy 2004;34:520-6. - PubMed
-
- Kemp AS. Atopic eczema: its social and financial costs. J Paediatr Child Health 1999;35:229-31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical