

An adaptive-duration version of the PVT accurately tracks changes in psychomotor vigilance induced by sleep restriction
- PMID: 22294809
- PMCID: PMC3250358
- DOI: 10.5665/sleep.1620
An adaptive-duration version of the PVT accurately tracks changes in psychomotor vigilance induced by sleep restriction
Abstract
Study objectives: The Psychomotor Vigilance Test (PVT) is a widely used assay of behavioral alertness sensitive to the effects of sleep loss and circadian misalignment. The standard 10-minute duration of the PVT is often considered impractical for operational or clinical environments. Therefore, we developed and validated an adaptive-duration version of the PVT (PVT-A) that stops sampling once it has gathered enough information to correctly classify PVT performance.
Design: Repeated-measures experiments involving 10-minute PVT assessments every 2 hours across both acute total sleep deprivation (TSD) and 5 days of chronic partial sleep deprivation (PSD).
Setting: Controlled laboratory environment.
Participants: Seventy-four healthy subjects (34 women), aged 22 to 45 years.
Interventions: A TSD experiment involving 33 hours awake (n = 31 subjects), and a PSD experiment involving 5 nights of 4 hours time in bed (n = 43 subjects).
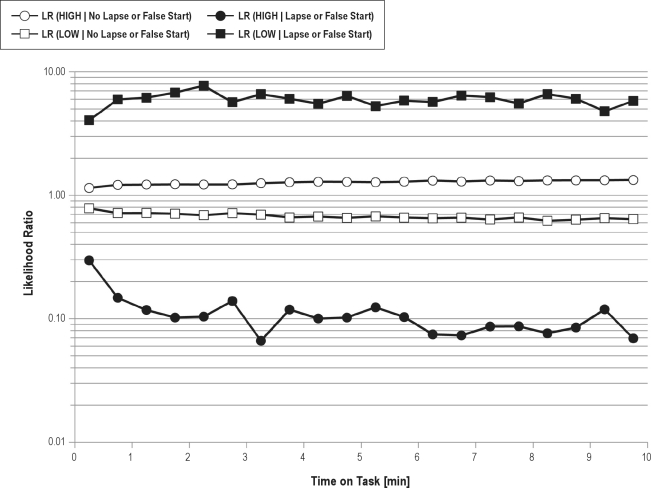
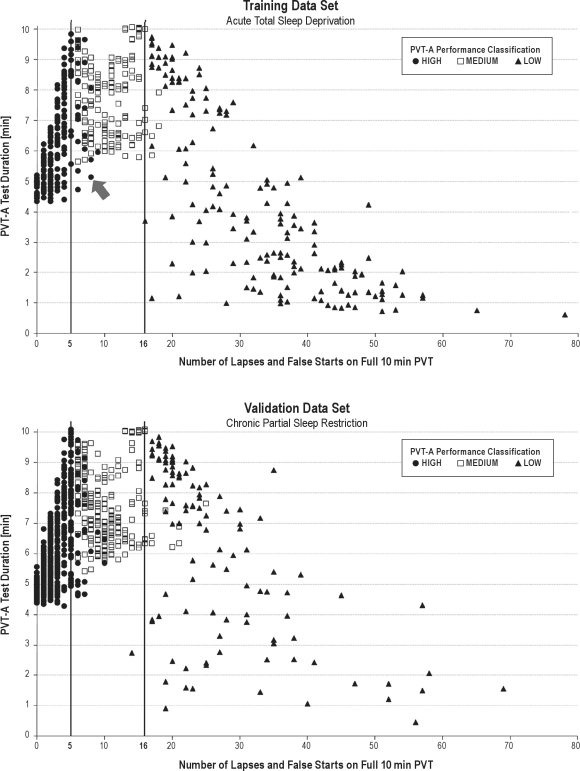
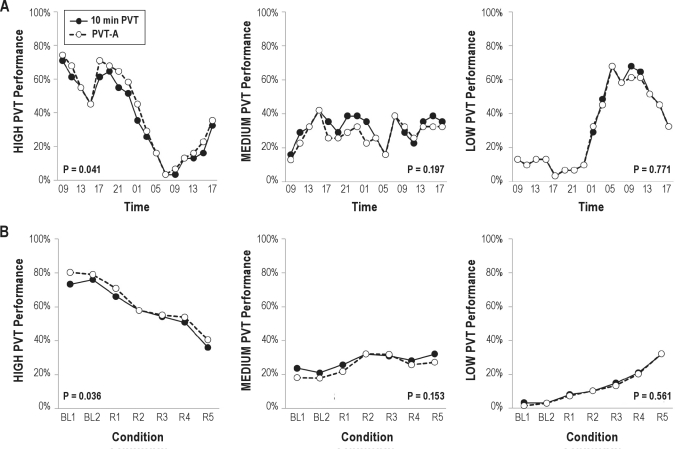
Measurements and results: The PVT-A algorithm was trained with 527 TSD test bouts and validated with 880 PSD test bouts. Based on our primary outcome measure "number of lapses (response times ≥ 500 ms) plus false starts (premature responses or response times < 100 ms)," 10-minute PVT performance was classified into high (≤ 5 lapses and false starts), medium (> 5 and ≤ 16 lapses and false starts), or low (> 16 lapses and false starts). The decision threshold for PVT-A termination was set so that at least 95% of training data-set tests were classified correctly and no test was classified incorrectly across 2 performance categories (i.e., high as low or low as high), resulting in an average test duration of 6.0 minutes (SD 2.4 min). In the validation data set, 95.7% of test bouts were correctly classified, and there were no incorrect classifications across 2 categories. Agreement corrected for chance was excellent (κ = 0.92). Across the 3 performance categories, sensitivity averaged 93.7% (range 87.2%-100%), and specificity averaged 96.8% (range 91.6%-99.9%). Test duration averaged 6.4 minutes (SD 1.7 min), with a minimum of 27 seconds.
Conclusions: We developed and validated a highly accurate, sensitive, and specific adaptive-duration version of the 10-minute PVT. Test duration of the adaptive PVT averaged less than 6.5 minutes, with 60 tests (4.3%) terminating after less than 2 minutes, increasing the practicability of the test in operational and clinical settings. The adaptive-duration strategy may be superior to a simple reduction of PVT duration in which the fixed test duration may be too short to identify subjects with moderate impairment (showing deficits only later during the test) but unnecessarily long for those who are either fully alert or severely impaired.
Keywords: PVT; alertness; attention; lapse; psychomotor vigilance; response speed; response time; sensitivity; sleep deprivation.
Figures
References
-
- Barger LK, Cade BE, Ayas NT, et al. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125–34. - PubMed
-
- Dinges DF. An overview of sleepiness and accidents. J Sleep Res. 1995;4:4–14. - PubMed
-
- Finkel KJ, Searleman AC, Tymkew H, et al. Prevalence of undiagnosed obstructive sleep apnea among adult surgical patients in an academic medical center. Sleep Med. 2009;10:753–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
