

doi: 10.4061/2011/107981.
Epub 2011 Sep 4.
Breast conservation surgery: state of the art
Affiliations
- PMID: 22295209
- PMCID: PMC3262560
- DOI: 10.4061/2011/107981
Item in Clipboard
Breast conservation surgery: state of the art
Int J Breast Cancer.
2011.
Abstract
Breast conservation surgery is available to the vast majority of women with breast cancer. The combination of neoadjuvant therapies and oncoplastic surgical techniques allows even large tumours to be managed with a breast-conserving approach. The relationship between breast size and the volume of tissue to be excised determines the need for volume displacement or replacement. Such an approach can also be used in the management of carefully selected cases of multifocal or multicentric breast cancer. The role of novel techniques, such as endoscopic breast surgery and radiofrequency ablation, is yet to be precisely defined.
Figures
(a) This patient had previously undergone a central wide local excision and nipple reconstruction at the age of 47. Although the contour of the right breast is similar to that of the left, there is a relative lack of projection and the breast has a blunted appearance. (b) Autologous fat transfer, in the form of lipomodelling, successfully fills the defect from previous surgery. The patient also received a subdermal silicone areola prosthesis to improve projection of the reconstructed nipple.

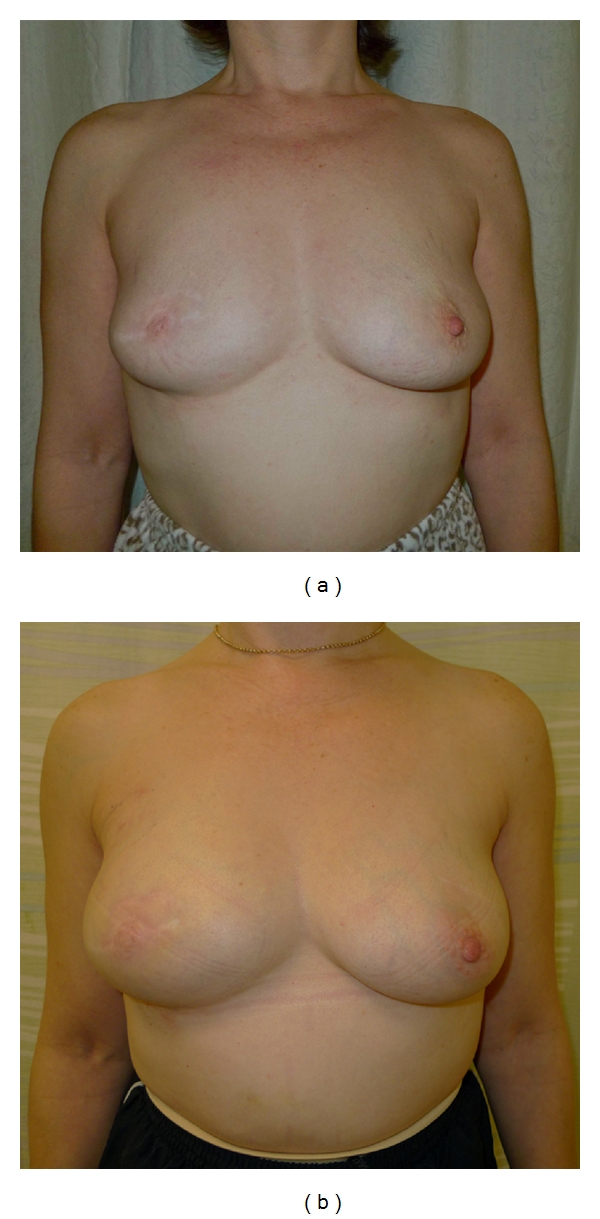
This patient presented with a 1 cm tumour located in the upper inner quadrant of the right breast. The tumour was excised via a periareolar incision and the remaining breast tissue was mobilised to close the defect. The round block technique ensured that the nipple-areolar complex remained in the correct position.
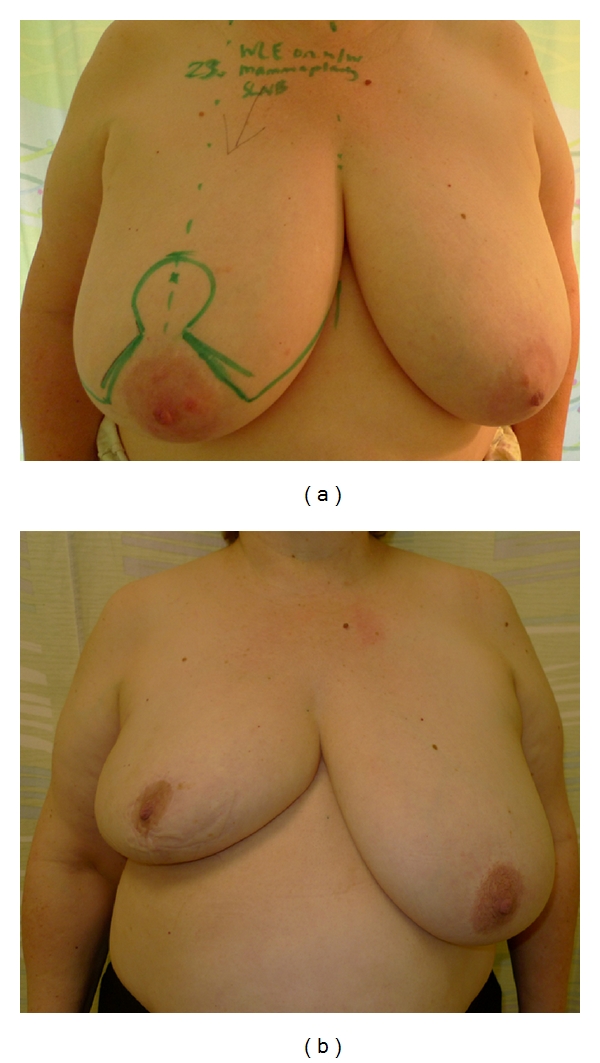
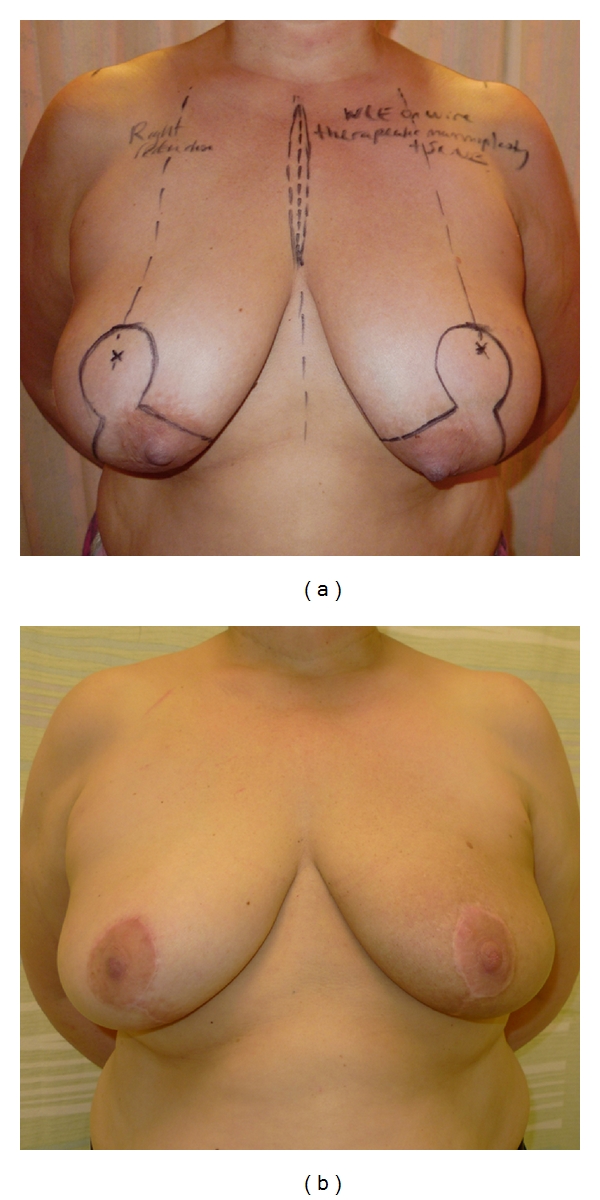
(a) This 63-year-old patient with large ptotic breasts presented with a tumour in the right breast. The skin markings show the planned incisions for a therapeutic inverted-T mammoplasty. (b) Postoperative images of the same patient after completion of adjuvant chemotherapy and prior to commencing radiotherapy. The inverted-T mammoplasty gives a satisfactory result and is in proportion to the patient's body habitus. Reduction mammoplasty of the contralateral breast, to improve symmetry, is planned to be performed six months after completion of adjuvant radiotherapy.
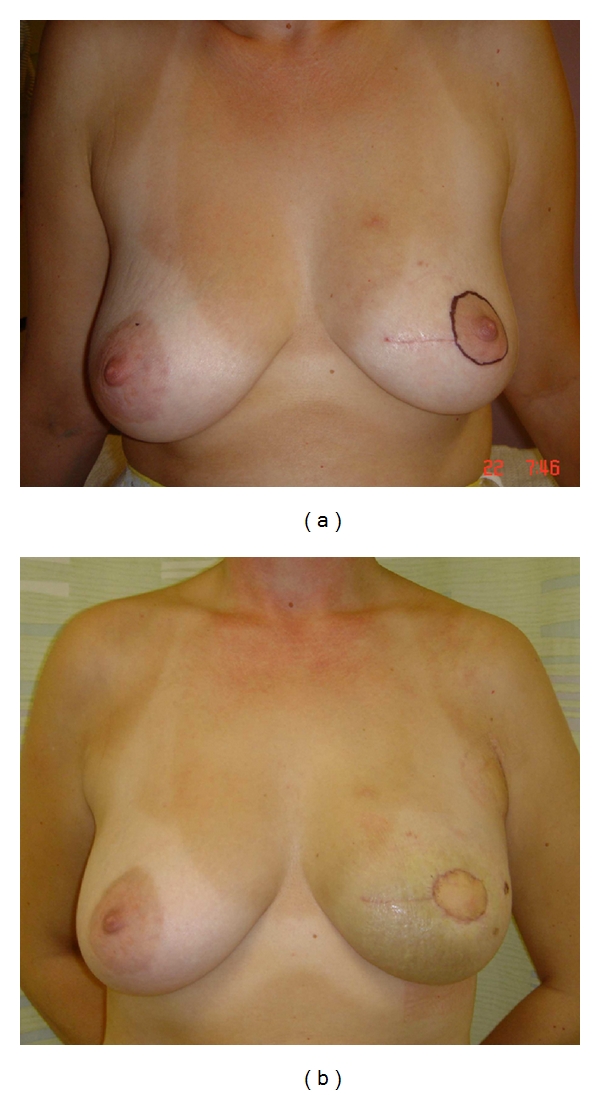
(a) This 41-year-old patient had previously undergone wide local excision of a tumour in the left breast. The lateral margin was involved, necessitating a further central wide local excision to include the nipple-areolar complex. (b) In view of the predicted loss of volume, a latissimus dorsi miniflap was utilised to both fill the resultant defect and also replace the skin of the areola. The volume of the partially reconstructed breast is very similar to that of the contralateral side, although postoperative swelling is apparent.
(a) This patient had previously undergone wide local excision and adjuvant radiotherapy for a cancer located in the lower inner quadrant of the left breast. The resulting defect causes significant distortion to the breast shape and nipple deviation toward the midline. (b) An omental flap was harvested laparoscopically in order to partially reconstruct the breast, achieving a high degree of symmetry with the contralateral breast.
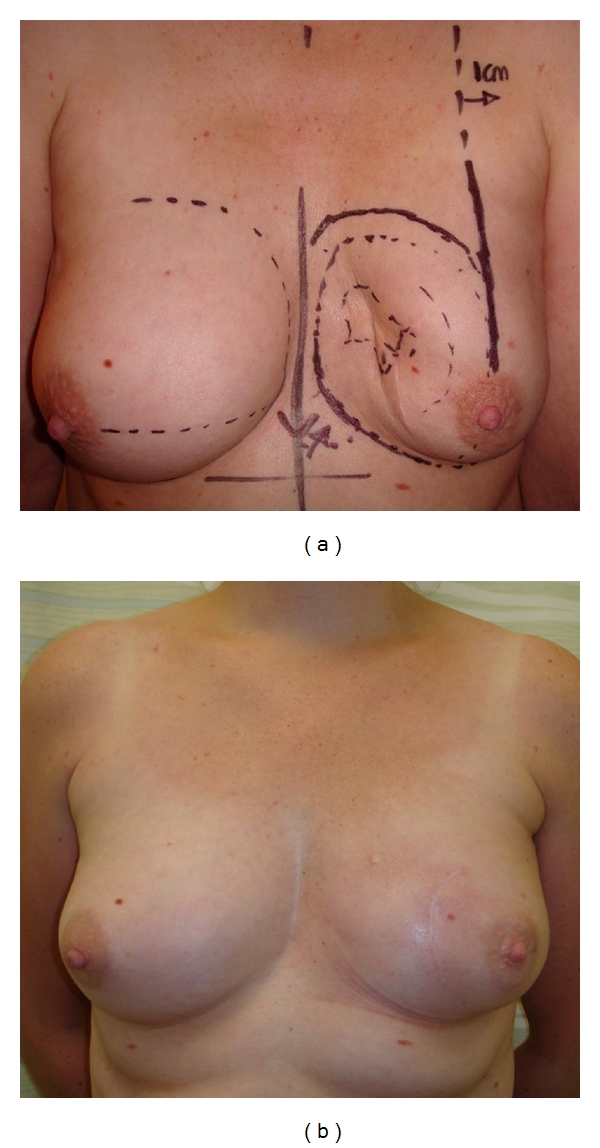
(a) This 51-year-old patient with large, ptotic breasts and nipple-areola complexes situated medial to the breast meridian presented with a left breast cancer. These images show the skin markings used to plan a therapeutic inverted-T mammoplasty and simultaneous contralateral reduction mammoplasty for symmetrisation. (b) Adjuvant radiotherapy to the left breast has resulted in mild changes in skin pigmentation but symmetry is still good with the contralateral breast being still satisfactory.
References
-
- Fisher B. Laboratory and clinical research in breast cancer—a personal adventure: the David A. Karnofsky memorial lecture. Cancer Research. 1980;40(11):3863–3874. - PubMed
-
- Valero VV, Buzdar AU, Hortobagyi GN. Locally advanced breast cancer. Oncologist. 1996;1(1-2):8–17. - PubMed
-
- Makris A, Powles TJ, Ashley SE, et al. A reduction in the requirements for mastectomy in a randomized trial of neoadjuvant chemoendocrine therapy in primary breast cancer. Annals of Oncology. 1998;9(11):1179–1184. - PubMed
-
- Baildam A, Bishop H, Boland G, et al. Oncoplastic breast surgery—a guide to good practice. The European Journal of Surgical Oncology. 2007;33(supplement 1):S1–S23. - PubMed
LinkOut - more resources
Full Text Sources
