

Patterns of cellular distribution with the sentinel node positive for breast cancer
- PMID: 22295237
- PMCID: PMC3262578
- DOI: 10.4061/2011/873987
Patterns of cellular distribution with the sentinel node positive for breast cancer
Abstract
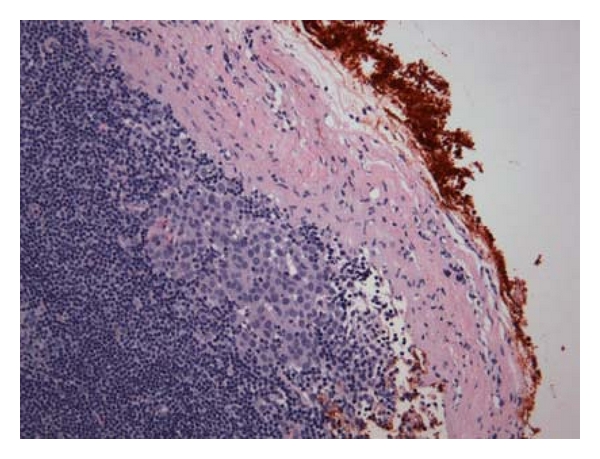
Background. Sentinel node biopsy (SNB) represents the standard of care in breast cancer axillary evaluation. Our study aims to characterize the patterns of malignant cell distribution within the sentinel nodes (SN). Methods. In a retrospective IRB-approved study, we examined the anatomic location of the nodal area with the highest radioactive signal or most intense blue staining (hot spot) and its distance from the metastatic foci. Results. 58 patients underwent SNB between January 2006 and February 2007. 12 patients with 19 positive SN were suitable for analysis. 4 (21%) metastases were located in the nodal hilum and 15 (79%) in the cortex. 6 (31%) metastases were found adjacent to the hotspot, and 9 (47%) within 4 mm of the hotspot. Conclusions. In our pilot series, SN metastases were within 4 mm of the hotspot in 78% of the cases. Pathologic analysis focused in that area may contribute to the more accurate identification of nodal metastases.
Figures

Similar articles
-
Sentinel node biopsy versus low axillary sampling in women with clinically node negative operable breast cancer.Breast. 2013 Dec;22(6):1081-6. doi: 10.1016/j.breast.2013.06.006. Epub 2013 Aug 13. Breast. 2013. PMID: 23948301 Clinical Trial.
-
Sentinel lymph node as a new marker for therapeutic planning in breast cancer patients.J Surg Oncol. 2004 Mar;85(3):102-11. doi: 10.1002/jso.20022. J Surg Oncol. 2004. PMID: 14991881 Review.
-
Determinants for non-sentinel node metastases in primary invasive breast cancer: a population-based cohort study of 602 consecutive patients with sentinel node metastases.BMC Cancer. 2019 Jun 25;19(1):626. doi: 10.1186/s12885-019-5823-x. BMC Cancer. 2019. PMID: 31238899 Free PMC article.
-
Evaluation of immunohistochemistry and multiple-level sectioning in sentinel lymph nodes from patients with breast cancer.Arch Pathol Lab Med. 2003 Jun;127(6):701-5. doi: 10.5858/2003-127-701-EOIAMS. Arch Pathol Lab Med. 2003. PMID: 12741893
-
[Prognostic and curative value of sentinel node in breast cancer. A 377 patients experience].Ann Ital Chir. 2010 Mar-Apr;81(2):103-11; discussion 112-3. Ann Ital Chir. 2010. PMID: 20726388 Review. Italian.
References
-
- Krag DN, Julian TB, Harlow SP, et al. NSABP-32: Phase III, randomized trial comparing axillary resection with sentinal lymph node dissection: a description of the trial. Annals of Surgical Oncology. 2004;11(3):208S–210S. - PubMed
-
- Krag DN, Anderson SJ, Julian TB, et al. Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial. The Lancet Oncology. 2010;11(10):927–933. - PMC - PubMed
-
- Land SR, Kopec JA, Julian TB, et al. Patient-reported outcomes in sentinel node-negative adjuvant breast cancer patients receiving sentinel-node biopsy or axillary dissection: National Surgical Adjuvant Breast and Bowel Project phase III protocol B-32. Journal of Clinical Oncology. 2010;28(25):3929–3936. - PMC - PubMed
-
- Olson JA, McCall LM, Beitsch P, et al. Impact of immediate versus delayed axillary node dissection on surgical outcomes in breast cancer patients with positive sentinel nodes: results from American College of Surgeons Oncology Group trials Z0010 and Z0011. Journal of Clinical Oncology. 2008;26(21):3530–3535. - PubMed
-
- Forbes RC, Pitchford C, Simpson JF, Balch GC, Kelley MC. Selective use of intraoperative touch prep analysis of sentinel nodes in breast cancer. American Surgeon. 2005;71(11):955–960. - PubMed
LinkOut - more resources
Full Text Sources
